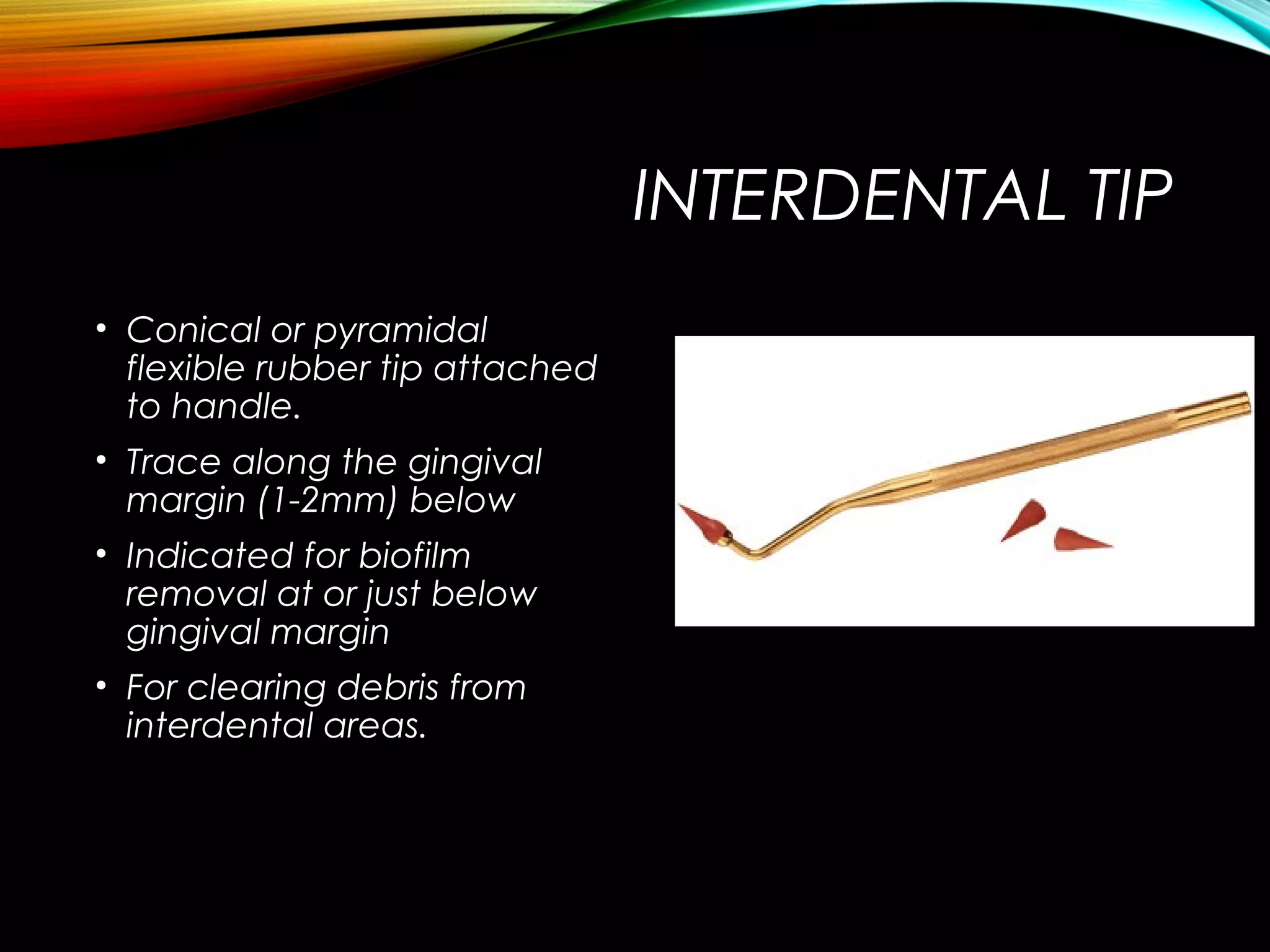
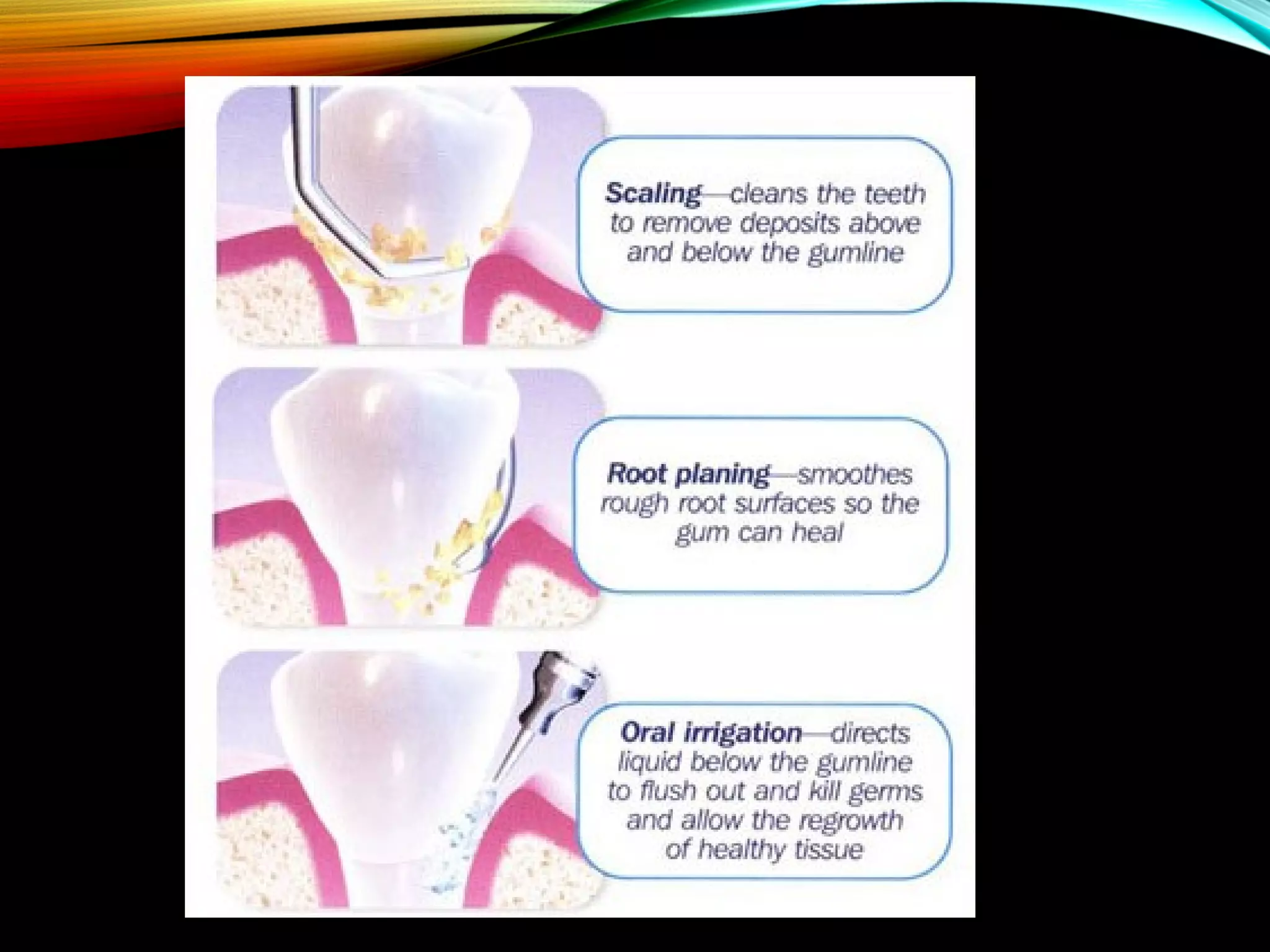
This document discusses various methods of mechanical plaque control, including toothbrushing, interdental cleaning aids, and oral irrigation. It provides details on the history and types of toothbrushes, proper brushing techniques, and the benefits of powered toothbrushes. Flossing and interdental brushes are described as important tools for cleaning between teeth. Gingival massage and oral irrigation are highlighted as adjuncts for removing plaque and bacteria. The conclusion emphasizes that daily mechanical plaque removal is key to disrupting plaque growth and maintaining oral health.

























































![PLAQUE CONTROL.ppt [Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrol-220827085644-ef330fe9-thumbnail.jpg?width=640&height=640&fit=bounds)

































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



