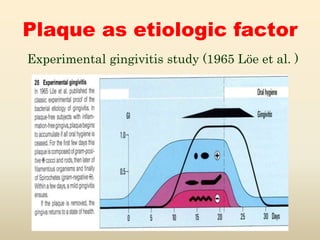
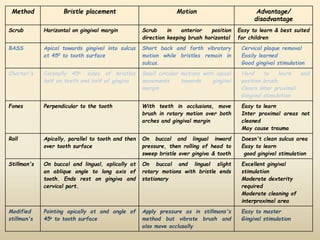
This document discusses mechanical plaque control methods including toothbrushing and interdental cleaning aids. It provides details on toothbrush design, different toothbrushing techniques like the Bass method and factors that influence brushing effectiveness. Powered toothbrushes and their advantages are also mentioned. The document further discusses dentifrices, their composition and role in aiding plaque removal and polishing teeth. Common abrasives, humectants and soaps used in dentifrices are outlined.















































































































![PLAQUE CONTROL.ppt [Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrol-220827085644-ef330fe9-thumbnail.jpg?width=640&height=640&fit=bounds)































