Download to read offline
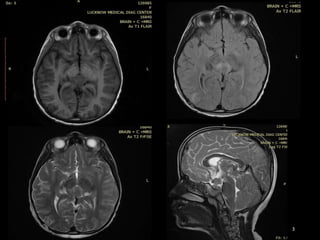

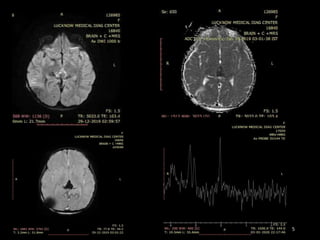
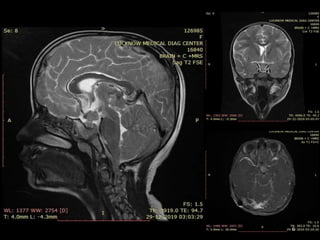
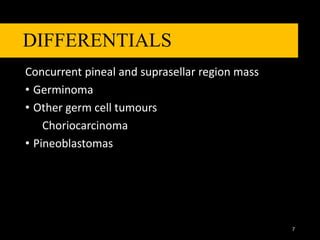

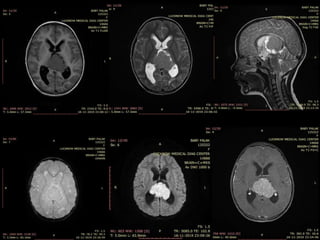


- A 9-year-old female patient presented with headache and numbness in the upper and lower limbs. Imaging showed a relatively well-defined heterogeneous enhancing mass lesion in the pineal region with a concurrent suprasellar mass and leptomeningeal spread. - The differential considerations included germinoma, pineoblastoma and choroid carcinoma. However, the likely diagnosis is germinoma given the age of the patient, pineal mass with concurrent suprasellar mass, and pattern of calcifications. Histopathological examination is awaited for confirmation.


































































