Download to read offline

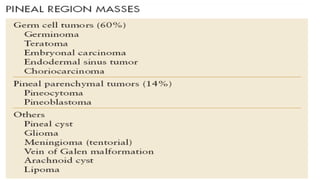
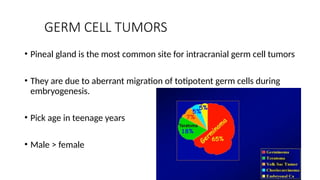
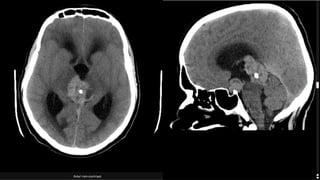
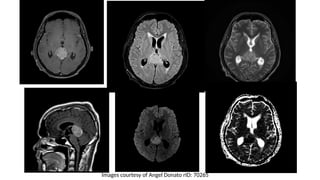
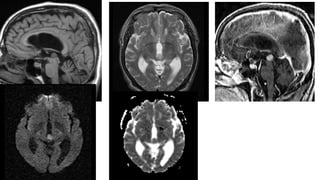

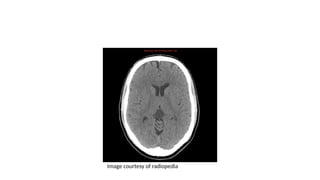
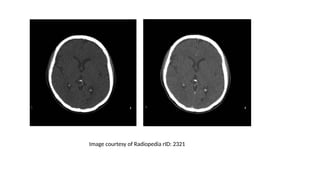
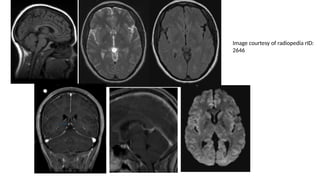

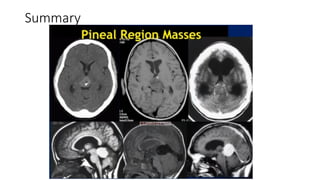
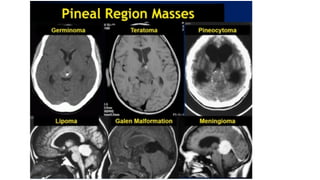

The document discusses pineal region masses, outlining the anatomy, imaging modalities, and types of tumors such as germ cell tumors, pineocytomas, and pineoblastomas. It highlights that germ cell tumors are the most common type found in children, with distinct imaging characteristics, while pineal cysts are frequently encountered as incidental findings. Additionally, it provides details on the clinical presentation, imaging findings on CT and MRI, and relevant references for further reading.














































