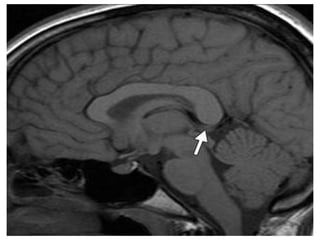
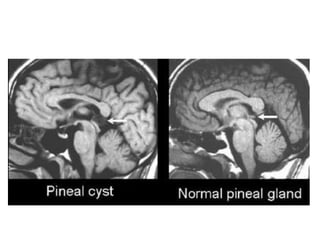
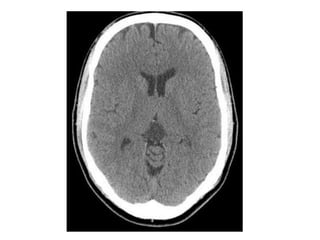
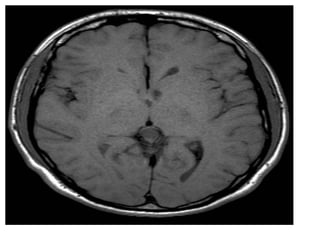
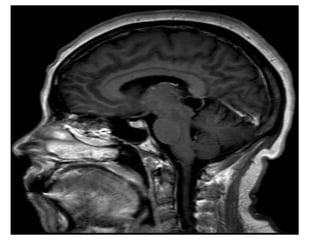
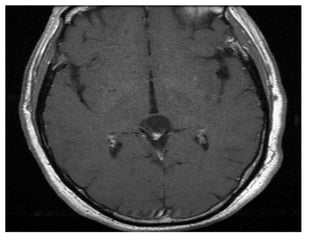
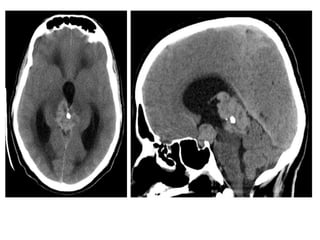
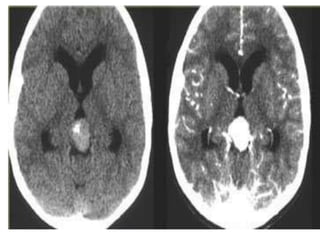
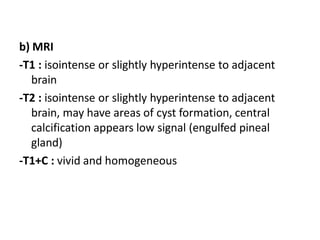
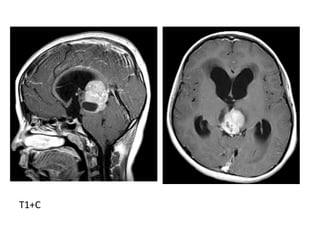
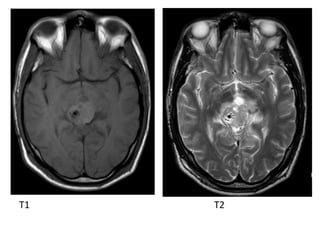
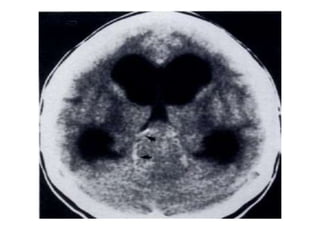
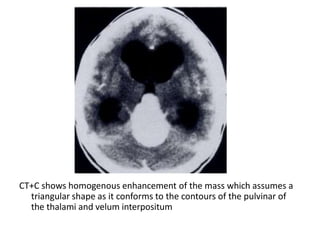
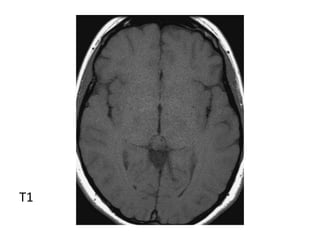
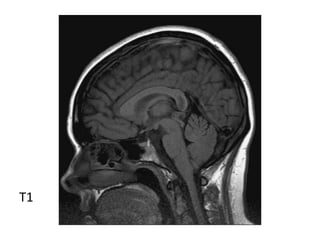
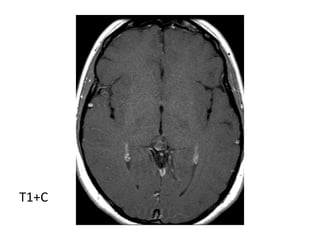
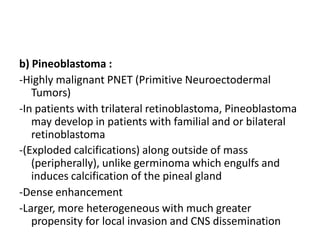
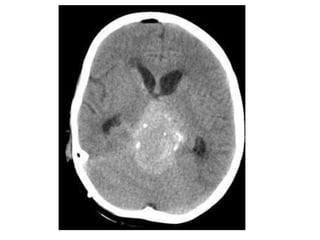
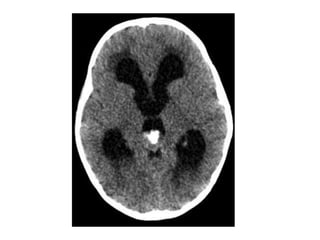
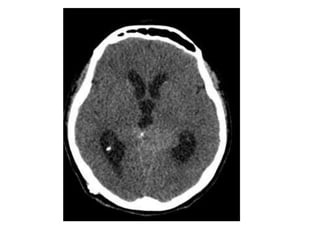
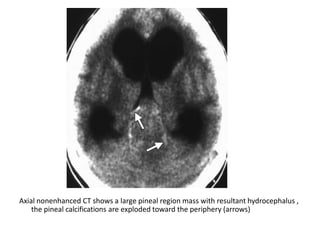
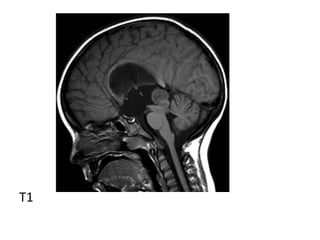
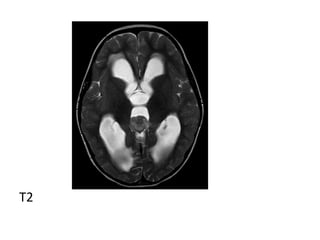
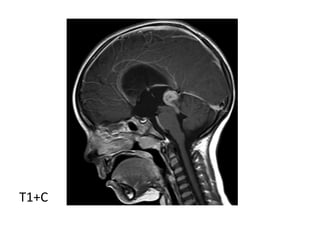
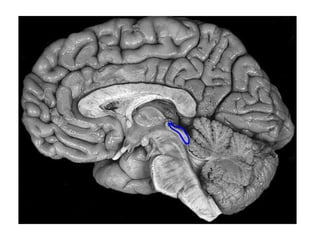
This document discusses masses that can occur in the pineal region. It describes benign cysts as common incidental findings, seen more often in younger women. Germ cell tumors are another common type and include germinomas, teratomas and others. Imaging can help differentiate these. Rarer parenchymal cell tumors include pineocytomas and pineoblastomas. Extrinsic masses such as gliomas, vein of Galen aneurysms, meningiomas and lipomas are also discussed along with their characteristic imaging features.