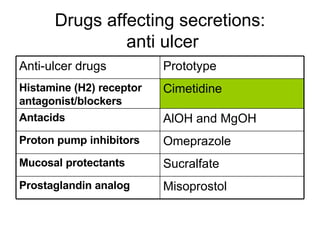
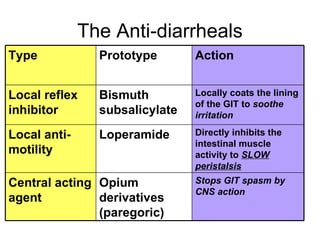
The document discusses drugs that affect the gastrointestinal system. It covers drugs that affect GI secretions like histamine receptor blockers, proton pump inhibitors, antacids, mucosal protectants and prostaglandin analogs. It provides details on the mechanisms of action, indications, side effects and nursing considerations for various classes of drugs including H2 receptor blockers, antacids, proton pump inhibitors and the mucosal protectant sucralfate.


























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



