Downloaded 138 times
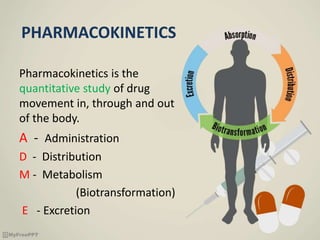
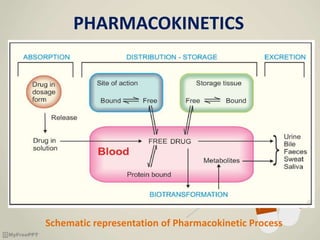
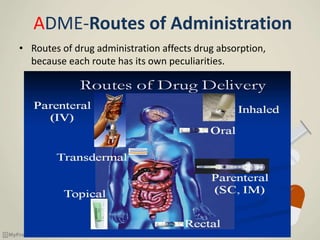
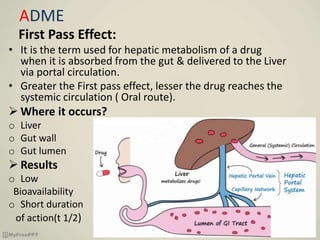
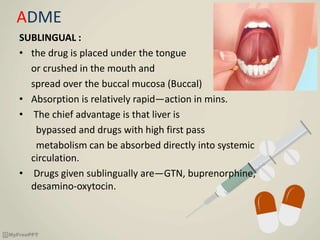
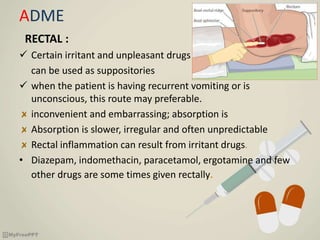
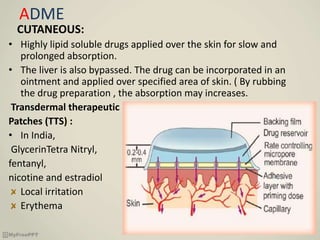
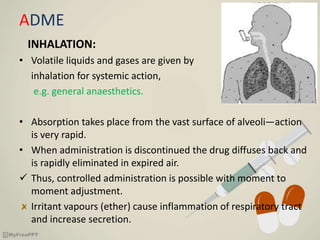

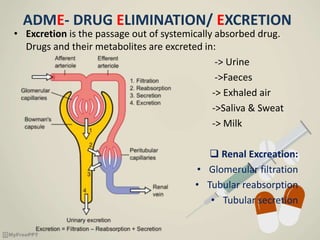


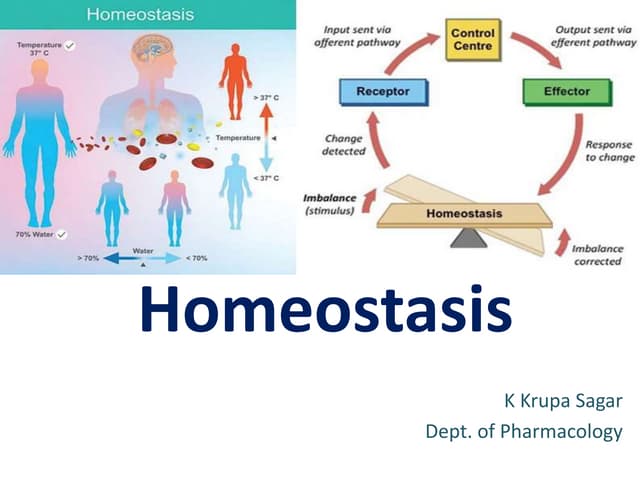
The document discusses drug nomenclature and pharmacokinetics. It explains that drugs have three categories of names - chemical, non-proprietary, and proprietary. It then describes the processes of absorption, distribution, metabolism, and excretion that make up a drug's pharmacokinetics. Absorption can occur through various routes of administration like oral, sublingual, rectal, and parenteral routes. Distribution and metabolism determine the amount of drug that reaches the systemic circulation. Excretion removes the drug from the body.