Downloaded 892 times



























































![Clozapine CLOZARIL®
Schizophrenia HLA-DQB1
Improved safety: pharmacogenetic testing, in parallel with WBC monitoring, avoid
prescription to patients with high agranulocytosis risk.
Test „„PGxPredict: Clozapine””
Tretinoin VESANOID® APL PML/RARD Improve drug efficacy and safety.
Disease confirmation by t(15;17) cytogenetic marker
Valproic acid
DEPAKENE®
Seizures
UCD deficiency
Confirm disease: consider evaluation of UCD before therapy with valproate
Only informational pharmacogenetic tests in drug label
Panitumumab
VECTIBIX®
Cetuximab
ERBITUX® mCRC
K-RAS Improve efficacy: clinical benefit limited to patients with nonmutated K-RAS.
Imatinib
GLEEVEC®
GIST
C-KIT
Improve drug efficacy: clinical benefit in patients carriers of the activating C-KIT
mutation
Busulfan
MYLERAN®
CML
Philadelphia chromosome Improve drug efficacy: responders are positives for Philadelphia chromosome (BCR-
ABL)
Capecitabine
XELODA®
CRC
DPD deficiency
Improve drug safety: decreased DPD and increased level of 5fluorouracil is associated
with severe toxicity (e.g., stomatitis, diarrhoea, neutropenia and neurotoxicity).
Primaquine Malaria G6PD
deficiency
Improve drug safety: avoid acute intravascular hemolytic reactions.
Isoniazid,
Pyrazinamide
TB
NAT
Improve drug safety: dose adjustements based on NATmetabolic status, for slow
acetylators and fast acetylators to avoid severe adverse reaction of peripheral
neuropathy, or lack of efficacy, respectively.
Erlotinib
TARCEVA® NSCLC EGFR mutations
Confirm disease (at least 10% of the cells are EGFR-positive) and response to EGFR
tyrosine kinase inhibitors
Lenalidomide
REVLIMID®
Myelodysplasic syndromes
Deletion of chromosome
5q
(del[5q])
Confirm disease: indicated to treat those with transfusion dependent anemia caused
by low- or intermediate-risk of myelodysplasic syndromes associated with 5q(del[5q])](https://image.slidesharecdn.com/pharmacogenomics-150711085249-lva1-app6892/75/Pharmacogenomics-70-2048.jpg)


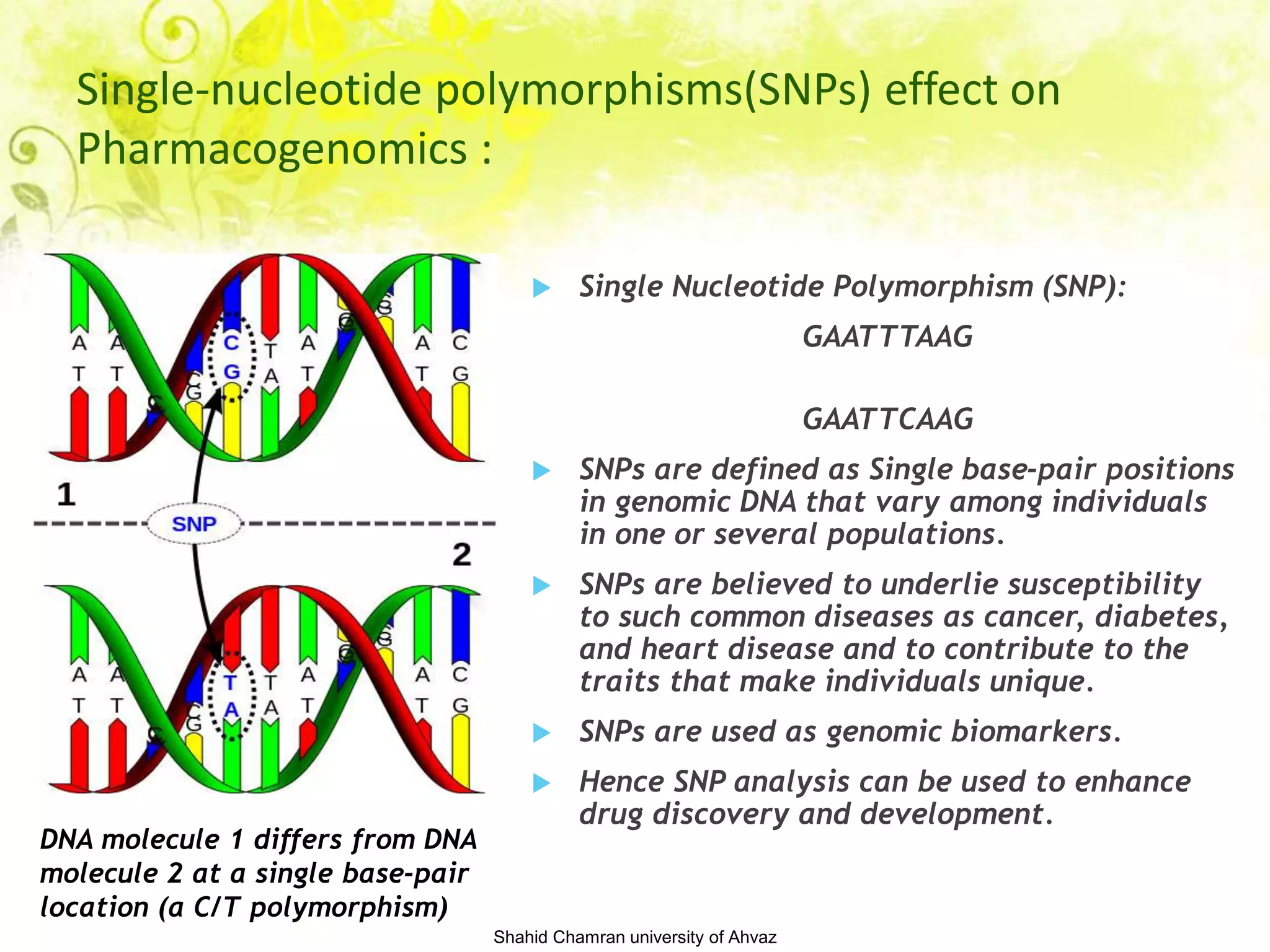
Pharmacogenomics is the study of how an individual's genetic inheritance affects their body's response to drugs. It involves studying the genetic basis for variability in drug efficacy and toxicity. The goal is to develop personalized medicine by understanding how genetic factors influence an individual's ability to metabolize and respond to drugs. Key factors that can vary between individuals include drug metabolizing enzymes, drug transporters, and drug targets. Genetic variations in these factors are associated with differences in drug efficacy or risk of adverse effects. Pharmacogenomic testing helps identify genetic polymorphisms that can predict drug response and dosing requirements.


























































































