Downloaded 383 times
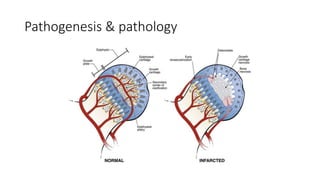
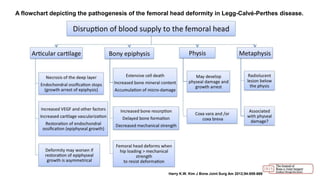
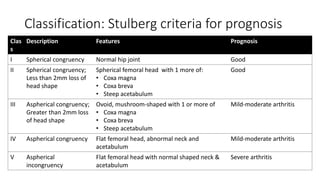
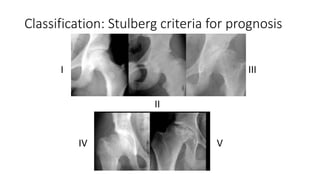
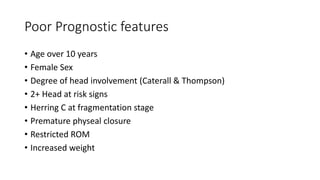
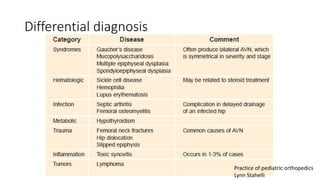


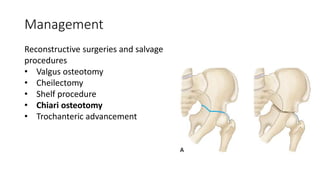
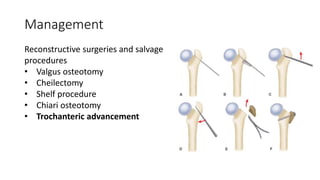

Legg-Calve-Perthes disease is a childhood condition caused by avascular necrosis of the femoral head. It leads to deformity of the femoral head and premature osteoarthritis. The exact cause is unknown but it is likely multifactorial, involving both genetic and environmental factors. Treatment depends on the age of the patient, extent of involvement, disease stage, and presence of head deformity. Younger patients often do well with non-operative treatment focusing on range of motion exercises, while older patients or those with more severe deformity may require surgical containment procedures like osteotomies to reshape the femoral head and acetabulum.































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



