This document provides information about Perthes disease, including:
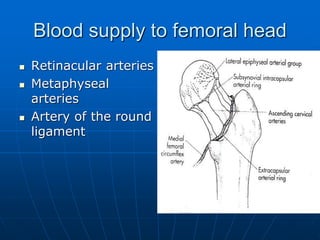
- It is a self-limiting condition caused by ischemia and necrosis of the femoral head, most common in children aged 4-8.
- Historical figures who studied the condition include Legg, Calve, and Perthes.
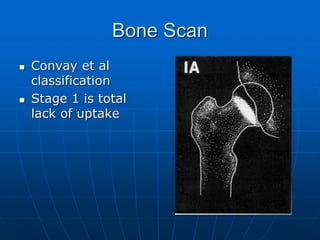
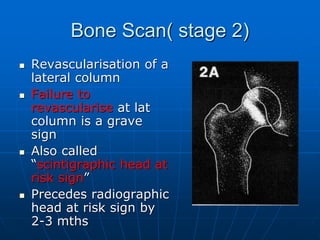
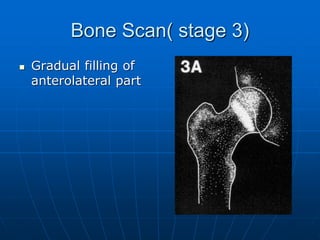
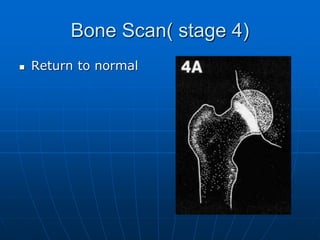
- The disease involves four stages: ischemic, fragmentation, reparative, and remodeling.
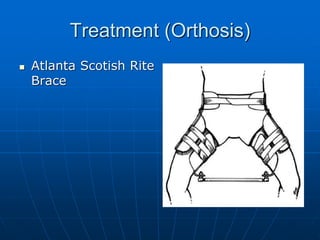
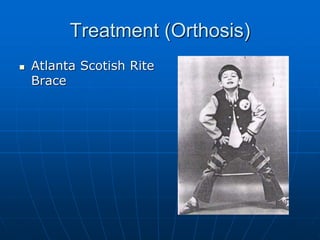
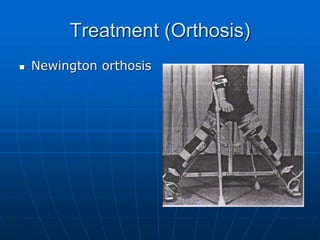
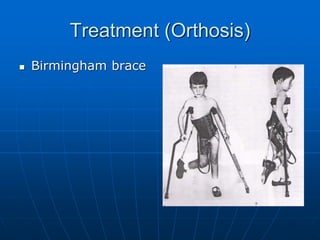
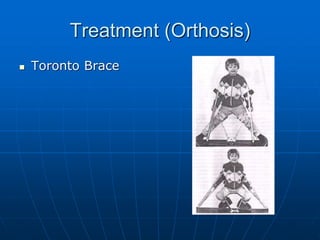
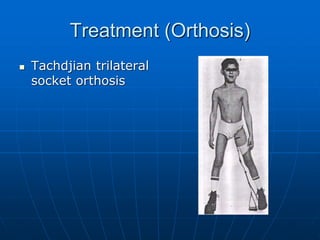
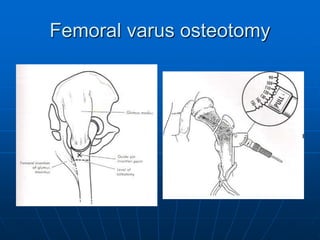
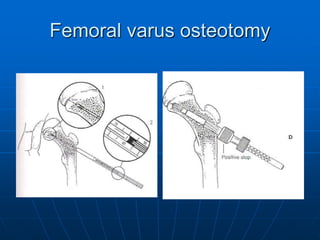
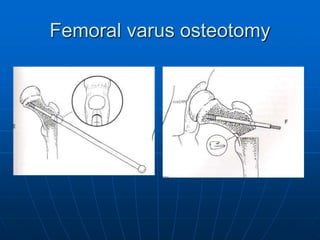
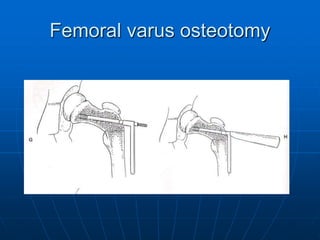
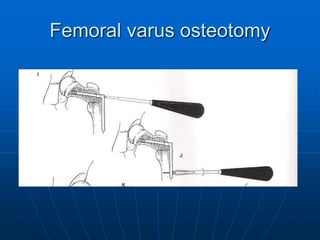
- Treatment aims to restore mobility, contain the femoral head, and allow weight bearing, through methods like bracing or osteotomies.
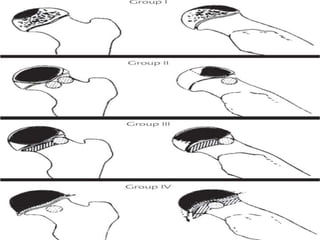
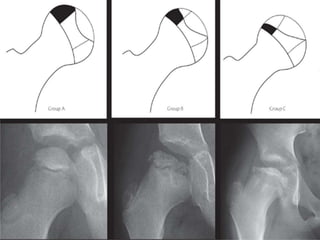
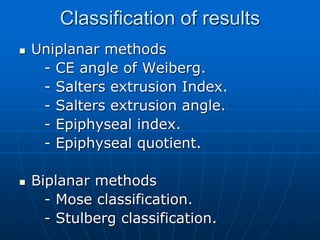
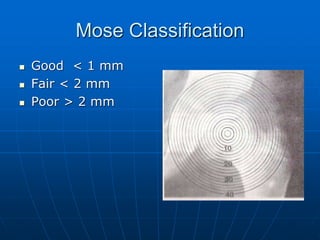
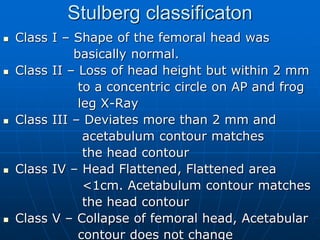
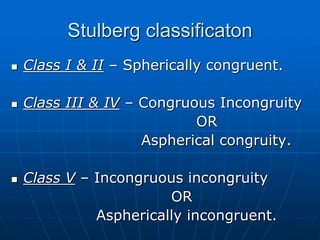
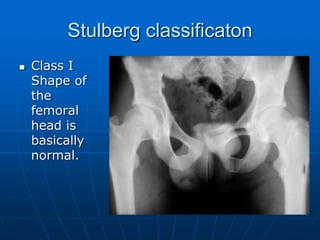
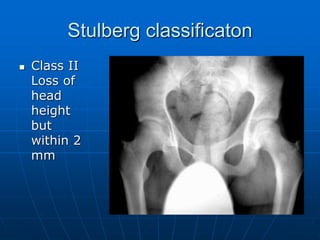
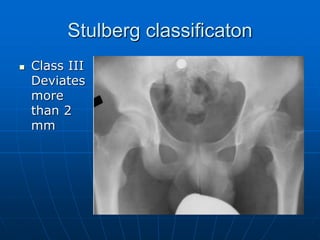
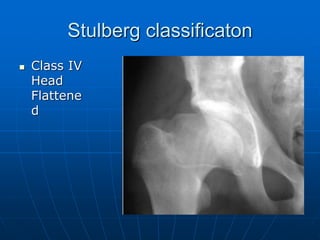
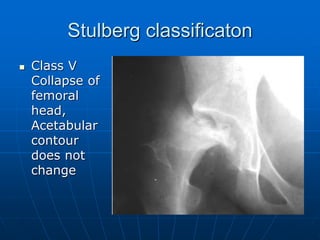
- Prognosis depends on factors like age of onset, extent of involvement, and classification system used to assess deformity and congruence.






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















