Downloaded 282 times






























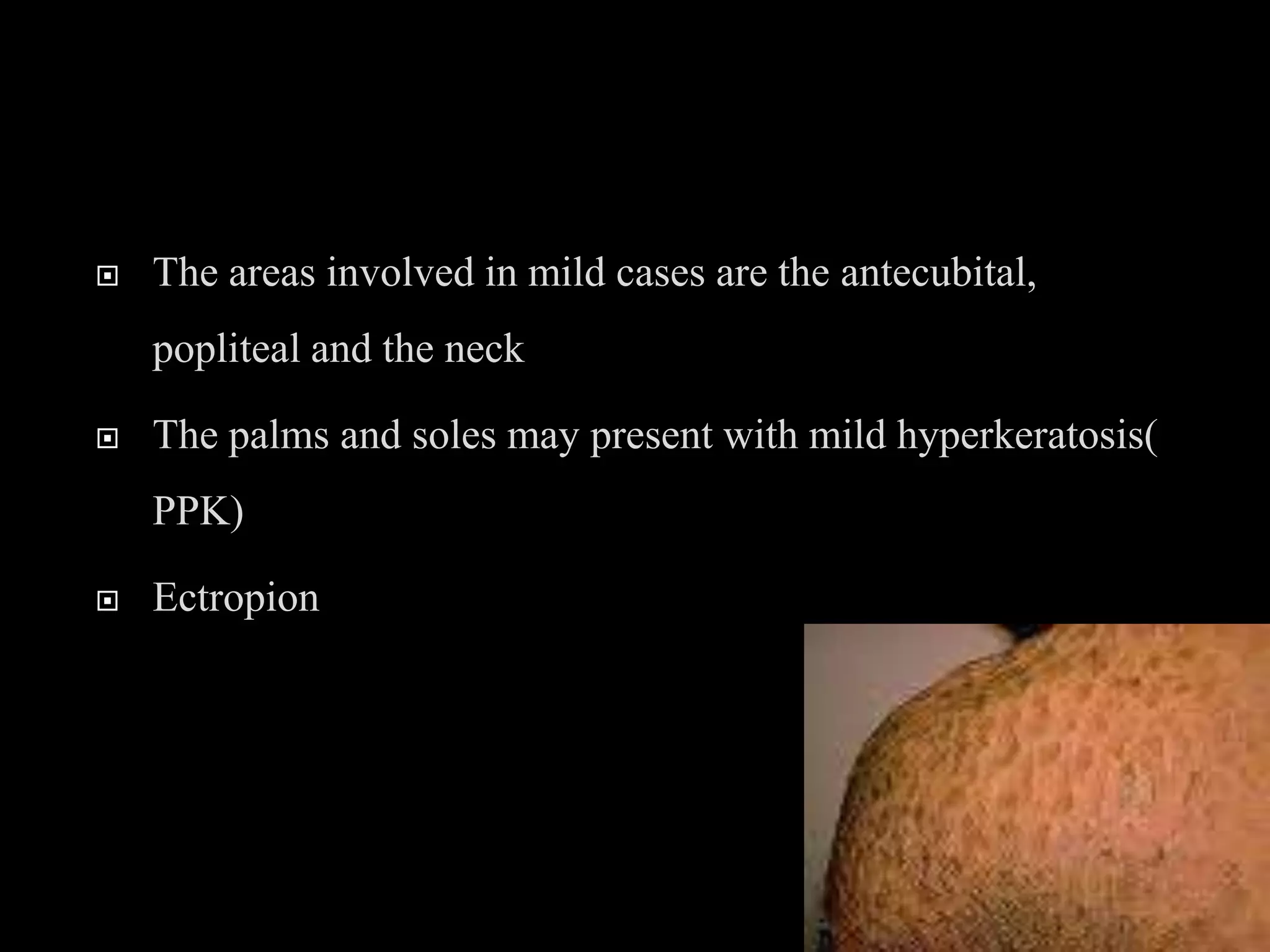









































The document discusses various types of ichthyosis, which are genetic skin disorders characterized by dry, thickened, scaly skin. It describes several specific types in detail, including ichthyosis vulgaris, X-linked ichthyosis, lamellar ichthyosis, and harlequin ichthyosis. Harlequin ichthyosis is the most severe form, where infants are born with thick armor-like plates covering their entire body, along with other abnormalities. Prenatal ultrasound findings and genetic testing are discussed which can help diagnose some severe types of ichthyosis in utero.




































































































