Downloaded 14 times
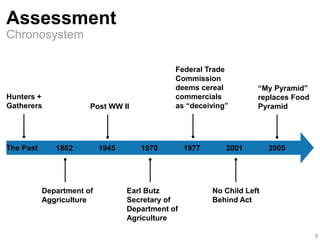
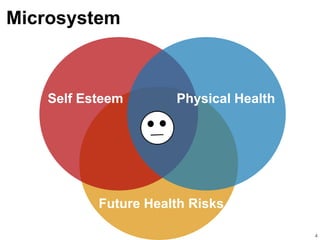
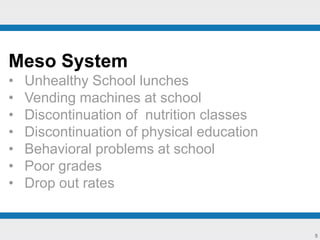
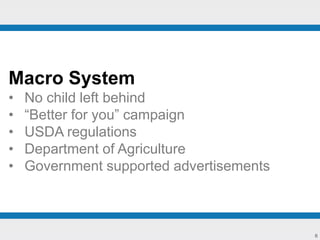
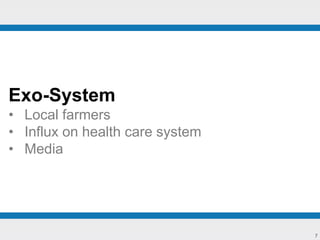
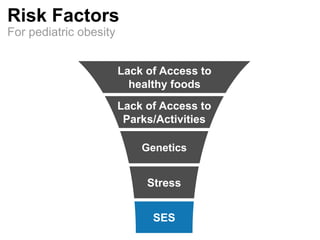





This document discusses pediatric obesity from multiple perspectives. It covers the chronosystem and risk factors for pediatric obesity. Interventions are discussed at various levels, including social, organizational, community, school-based, small group, and individual. Primary, secondary, universal, selective, and indicated prevention and promotion strategies are proposed. Personal, relational, and collective values related to pediatric obesity are also presented, including self-determination, caring, health, respect for diversity, participation, collaboration, community support, and social justice. The overall goal is to empower children and families to adopt healthy lifestyles and prevent pediatric obesity.

















































































