Downloaded 88 times






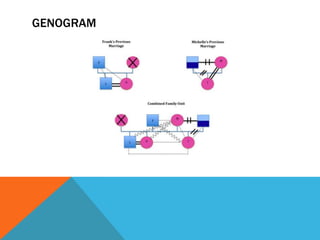
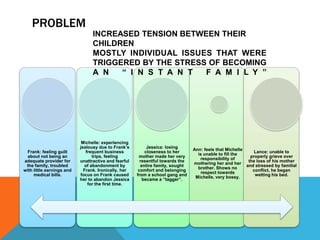
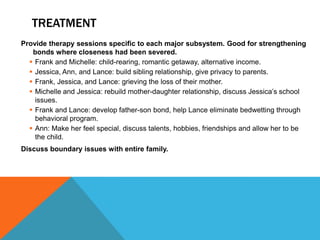

This document discusses the background and issues facing a blended family consisting of Frank, Michelle, Ann, Lance, and Jessica. Frank and Michelle recently married but each brought children from previous relationships. Problems arose from feelings of guilt, jealousy, resentment, and unresolved grief that were exacerbated by the stress of becoming an instant family. Therapy focused on strengthening relationships within each family subsystem through activities and discussions. This led to positive structural and behavioral changes where the family became better integrated and each individual member was able to address their specific issues.
































































































