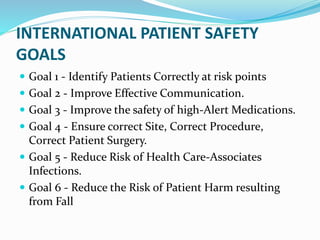
The document outlines international patient safety goals and guidelines for incident reporting. It discusses 6 main safety goals, including correctly identifying patients, improving communication, and reducing healthcare-associated infections. It also defines different types of incidents like near misses, adverse events, and sentinel events. For reporting, it specifies the immediate actions required and that all incidents must be reported to the quality department within 24 hours. The purpose is to distinguish between different adverse events to improve patient safety.