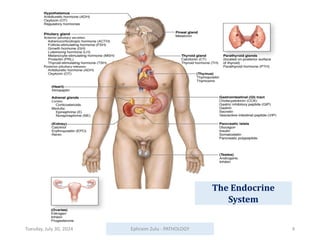
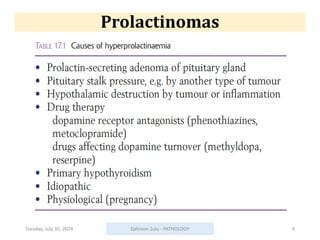
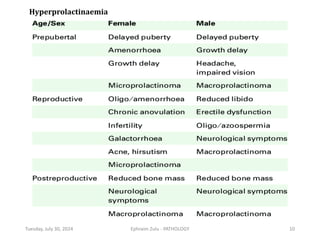
The document is a procedural lecture on endocrine pathology by Ephraim Imhotep Zulu, outlining various diseases affecting the endocrine system, including those of the pituitary, thyroid, parathyroid glands, pancreas, and adrenal glands. It covers key learning objectives related to the etiology, pathophysiology, and clinical features of common endocrine diseases, emphasizing conditions like hyperpituitarism, hyperthyroidism, and diabetes mellitus. The document also highlights rare diseases and syndromes like multiple endocrine neoplasia, providing insights into their distinct characteristics and implications.