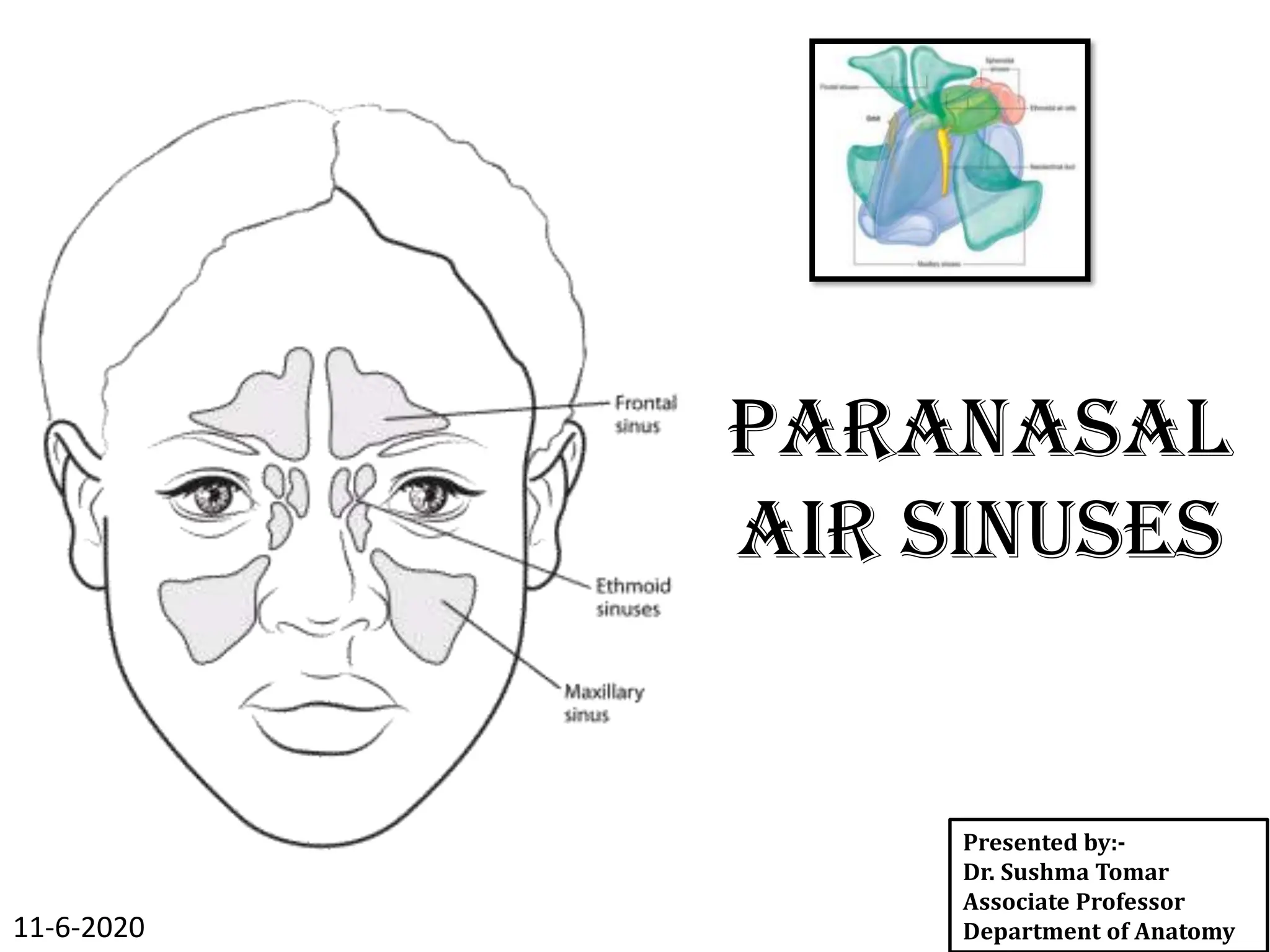
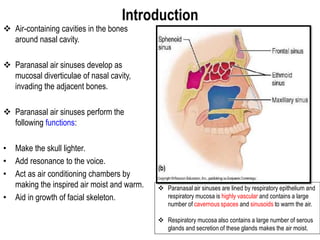
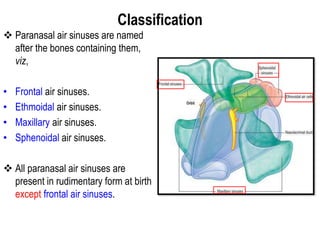
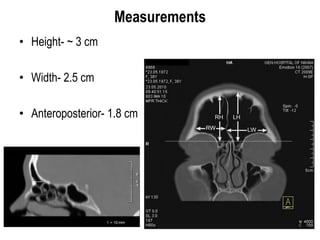
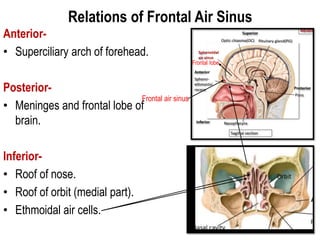
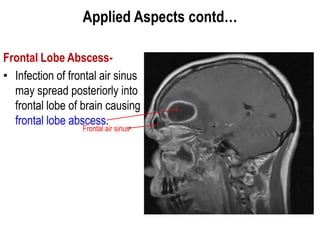
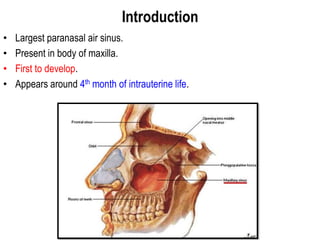
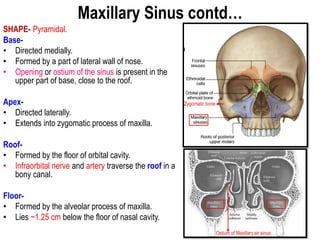
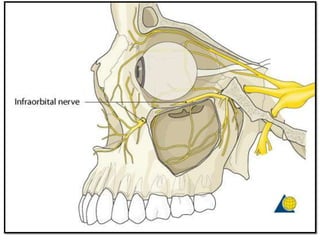
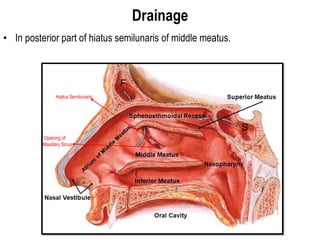
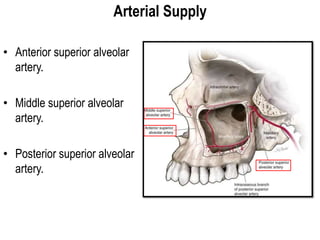
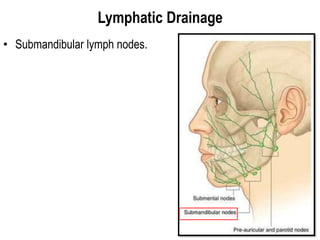
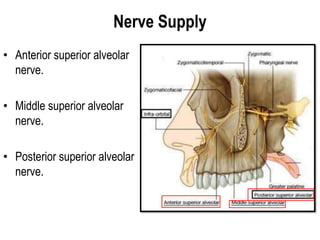
The document provides a comprehensive overview of paranasal air sinuses, including their classification, anatomy, and functions, such as lightening the skull and aiding voice resonance. Each type of sinus—frontal, maxillary, ethmoidal, and sphenoidal—is detailed with its drainage, supply, and clinical significance, particularly focusing on conditions like sinusitis and complications like abscesses and cellulitis. The relationships of these sinuses to surrounding structures and common surgical interventions for sinus issues are also discussed.