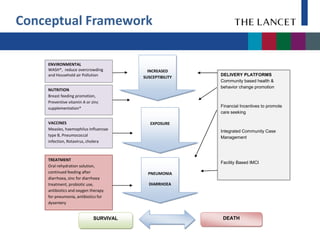
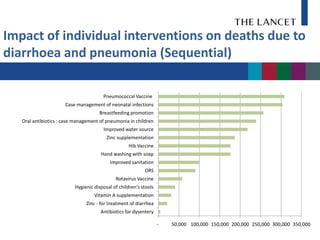
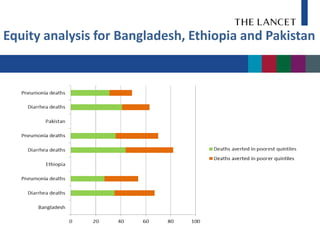
The document reviews effective interventions to reduce childhood pneumonia and diarrhoea deaths, analyzing 15 proven strategies and their impact on health outcomes across 75 countries. It emphasizes the importance of scaling up these interventions, projecting significant reductions in deaths if they are implemented effectively. Costs for these interventions are assessed, highlighting the need for equitable access and structural changes to ensure their success.