Downloaded 17 times
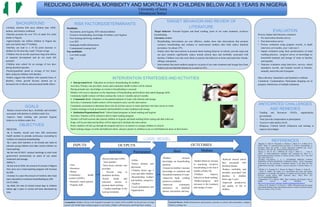
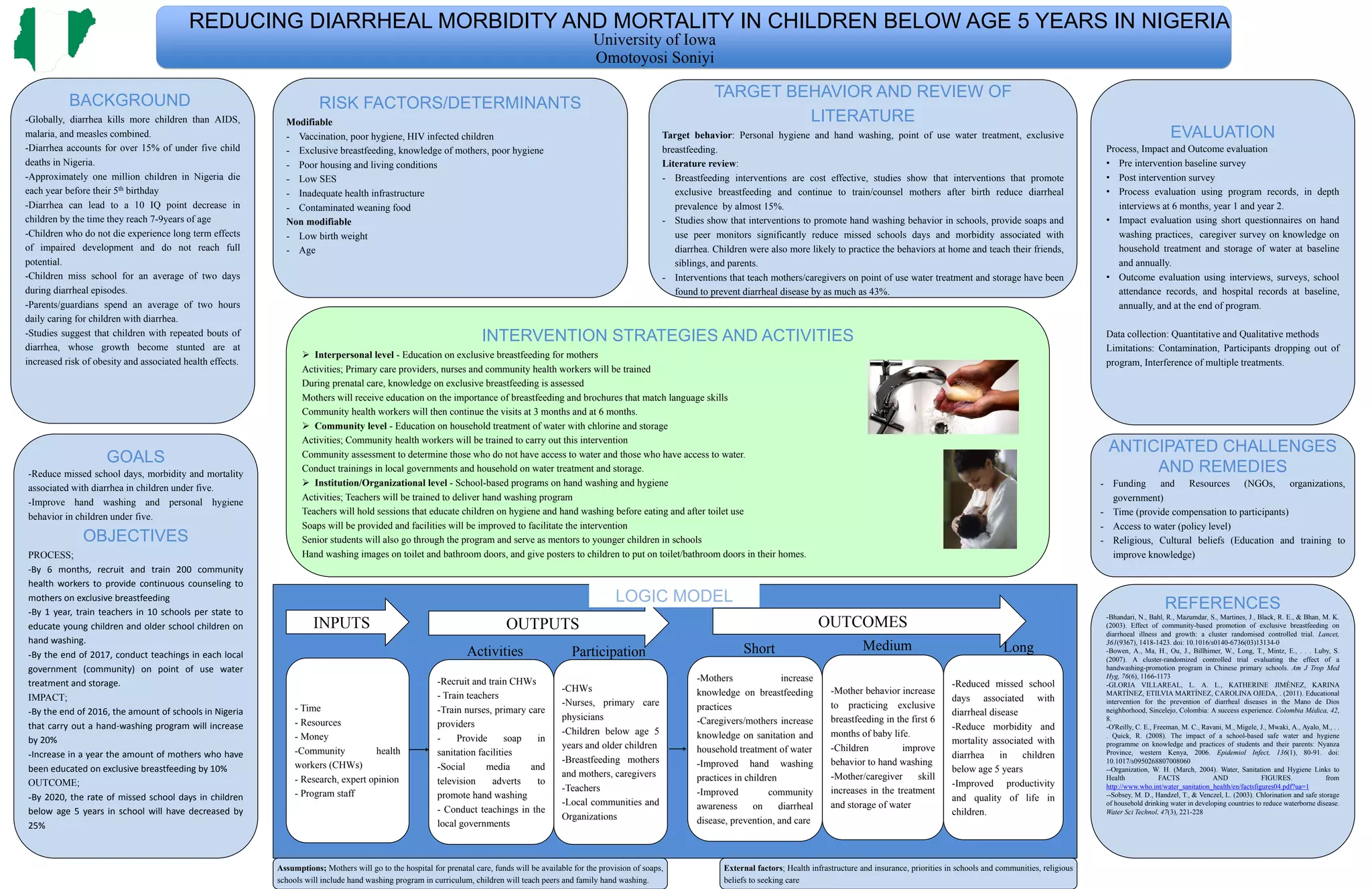

This document outlines a logic model for reducing diarrheal morbidity and mortality in children under 5 years old in Nigeria. It involves training community health workers, teachers, and healthcare providers to promote behaviors like exclusive breastfeeding, handwashing, and water treatment/storage. Evaluating the impact on knowledge, behaviors, and health outcomes will help reduce missed school/work days and the overall burden of diarrhea.





























































