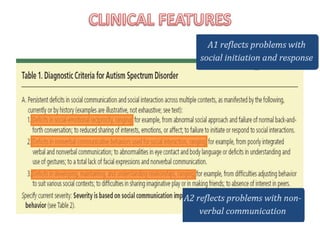
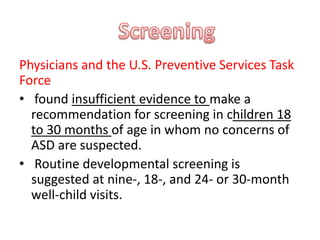
Autism spectrum disorder is characterized by difficulties with social communication and restricted behaviors. Screening with a validated tool at 18- and 24-month well-child visits can assist with early detection. Applied behavior analysis-based early intensive behavioral intervention delivered over an extended time frame improves cognitive ability, language, and adaptive skills. Medical management may also help target comorbid conditions, though behavioral intervention is usually most effective.