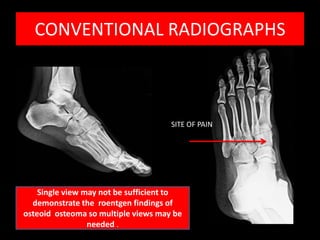
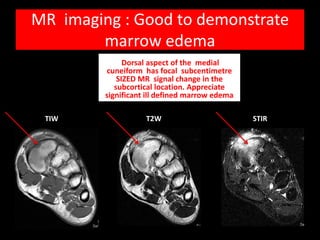
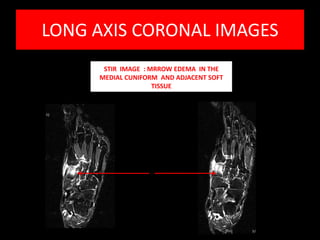
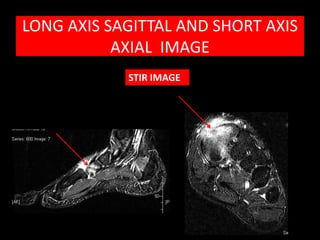
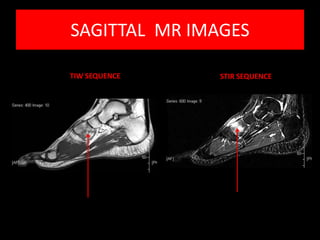
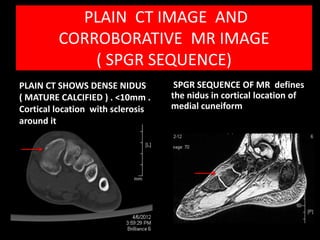
Osteoid osteoma is a benign bone tumor most common in young patients, typically causing pain worsened at night. Radiographs show a small lucent nidus surrounded by reactive sclerosis. CT precisely defines the calcified nidus. MRI demonstrates surrounding bone marrow edema. Treatment involves surgical excision or thermocoagulation of the nidus, providing effective pain relief. A multimodality imaging approach is useful to characterize the lesion and differentiate it from other causes of bone pain.