Download as PDF, PPTX


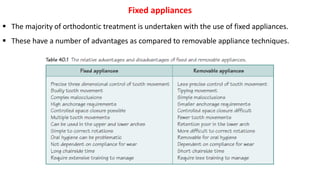
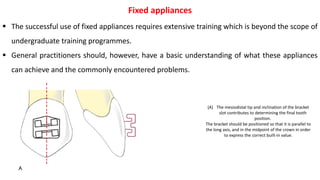

(1) Fixed appliances are commonly used in orthodontic treatment and have advantages over removable appliances. (2) The most commonly used fixed appliance is the pre-adjusted edgewise appliance, which positions teeth correctly through individual bracket placement. (3) Fixed appliances require extensive training to use properly but general dentists should understand what they can achieve and common problems.























































































