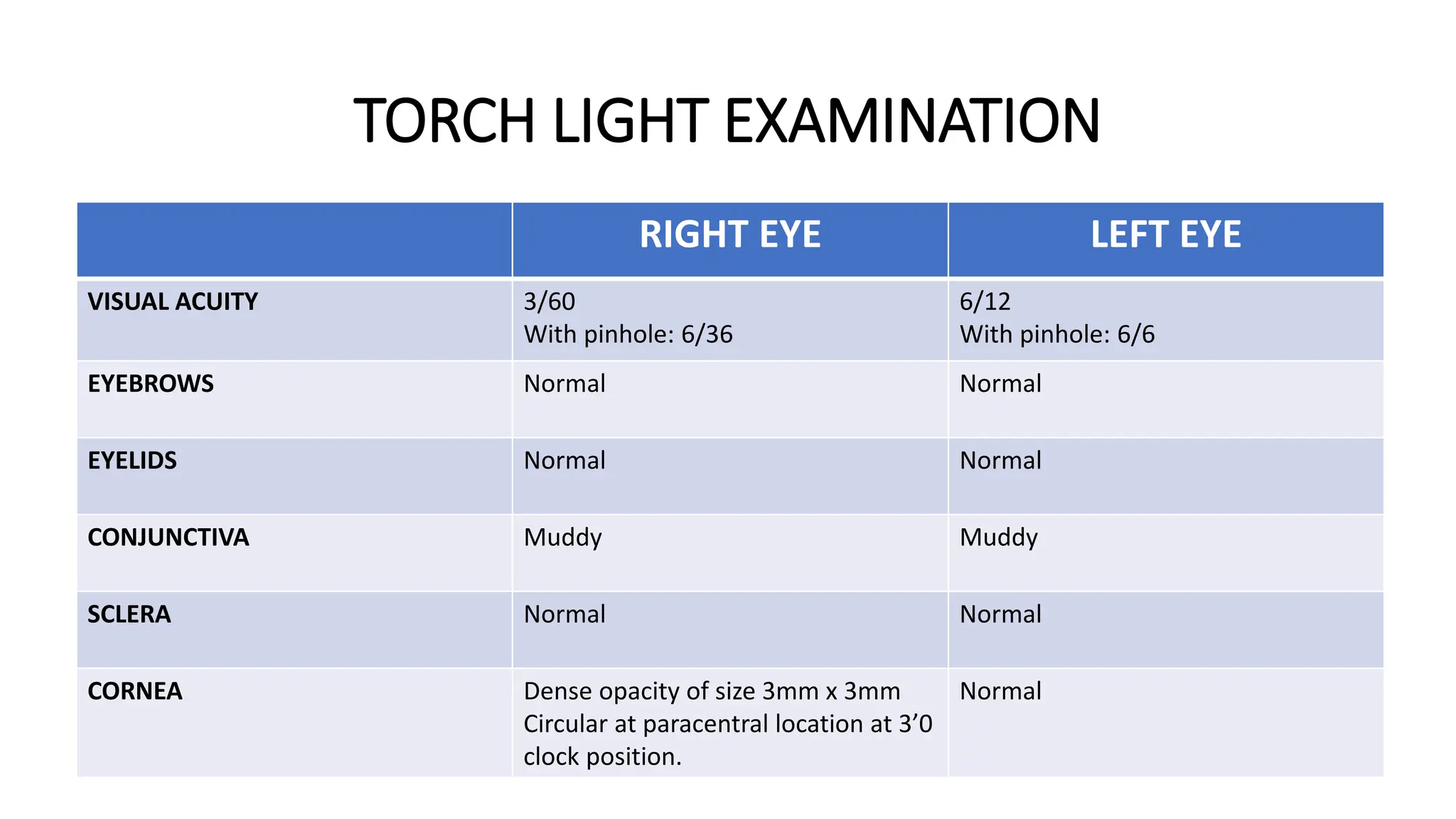
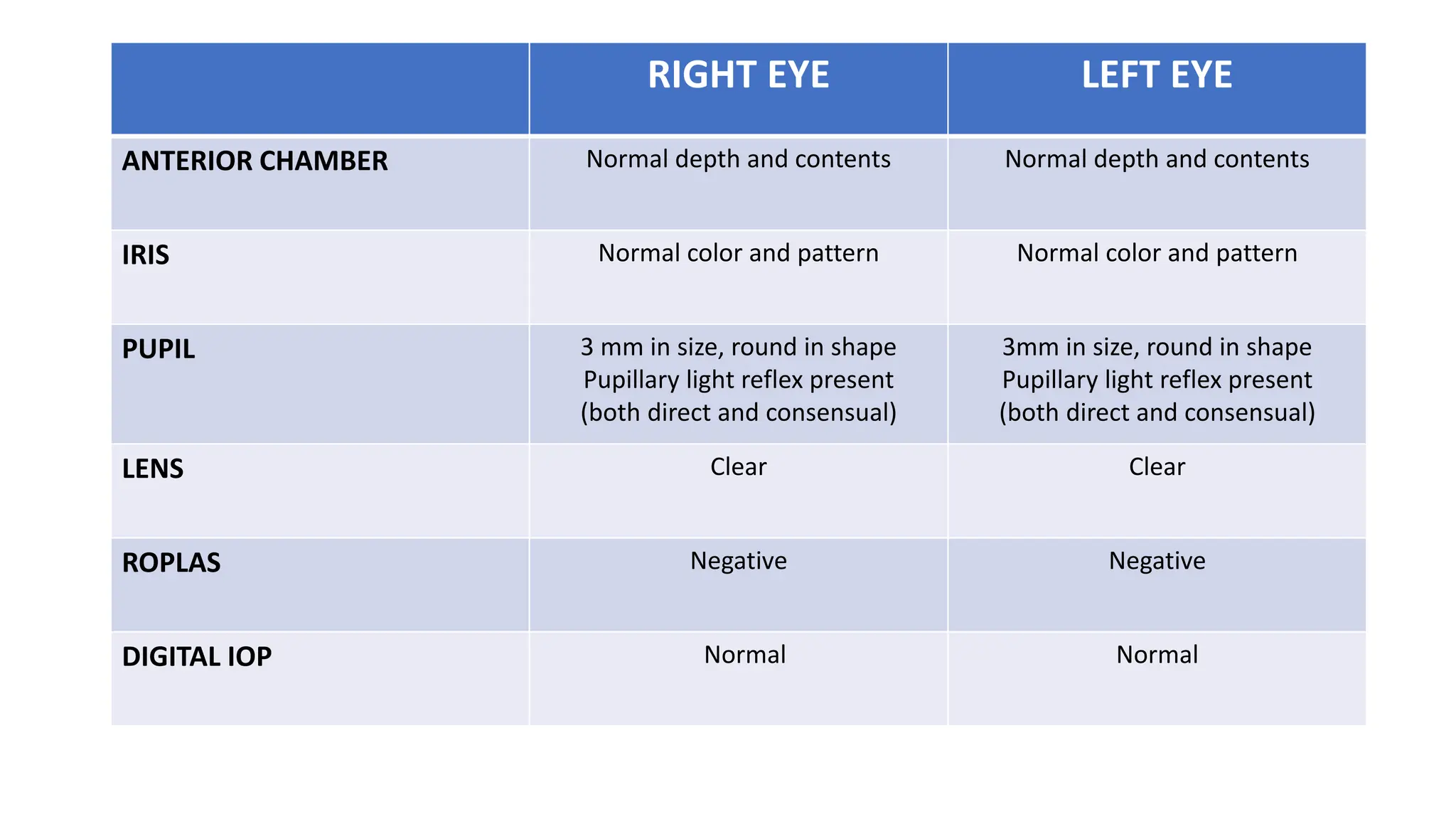
Mr. Arogya Das, a 55-year-old farm worker, presented with diminished vision in his right eye for 18 years following a traumatic injury in 2005. His ocular examination revealed a 3mm paracentral leucomatous corneal opacity affecting the pupillary area, and he is also a known case of diabetes and hypertension. Management options discussed include optical iridectomy and keratoplasty.