HISTORY OF PRESENTINGILLNESS
Patient was apparently alright 2 days back when he presented with pain
and swelling over right eye following trauma to right eye with a blunt
iron rod ,which was
• Sudden at onset
• gradually progressive in nature
• Associated with heaviness, watering in right eyes and gaze evoked
pain in right eye.
• Associated with redness, diplopia on right gaze.
5.
• History ofloss of concious for 5 mins
• Not associated with photophobia, coloured halos, discharge.
History of epistaxis present
6.
NEGATIVE HISTORY
• Noh/o nasal block, recurrent sinusitis, frequent respiratory tract infection,
epistaxis
• No h/o headache, projectile vomiting, seizures.
• No h/o postural variation, visible pulsations or change in colour of overlying skin
• No h/o fever, sweating, loss of appetite, arthralgia and weight loss.
• No h/o other swelling in the body
• No h/o radiation therapy or chemotherapy in the past
7.
PAST HISTORY
• Nopast history of ocular trauma or ocular surgery.
• No history of hypertension, diabetes mellitus, tuberculosis, and
Cerebrovascular disease,coronary artery disease,Epilepsy,drug
allergy,antiretroviral therapy,
• No history of any other systemic diseases.
8.
PERSONAL HISTORY
• Mixeddiet
• Normal sleep
• Regular bowel and bladder habit.
• Alcoholic occasionally, Non-smoker
• No h/o allergy or atopy
GENERAL PHYSICAL EXAMINATION
•Conscious,well oriented to time, place and person
•Moderately built, well nourished
•NO pallor, icterus, cyanosis, clubbing or generalised
lymphadenopathy
•PR=74/min, Regular, hypervolemic, equal on both sides
•BP: 150/90MMHG IN THE RIGHT ARM IN THE SITTING
POSITION
•RESPIRATORY RATE:12/MIN
•spO2-99%in room air
11.
SYSTEMIC EXAMINATION
• CVS:S1S2 HEARD, NO MURMUR
• RS: B/L AIR ENTRY, NORMAL VESICULAR BREATH SOUND+
• Temperature : afebrile
• P/A: SOFT, NON TENDER, NO ORGANOMEGALY
• No regional Lymph nodes enlargement (preauricular,
submandibular)
• Central and Peripheral Nervous System-Normal
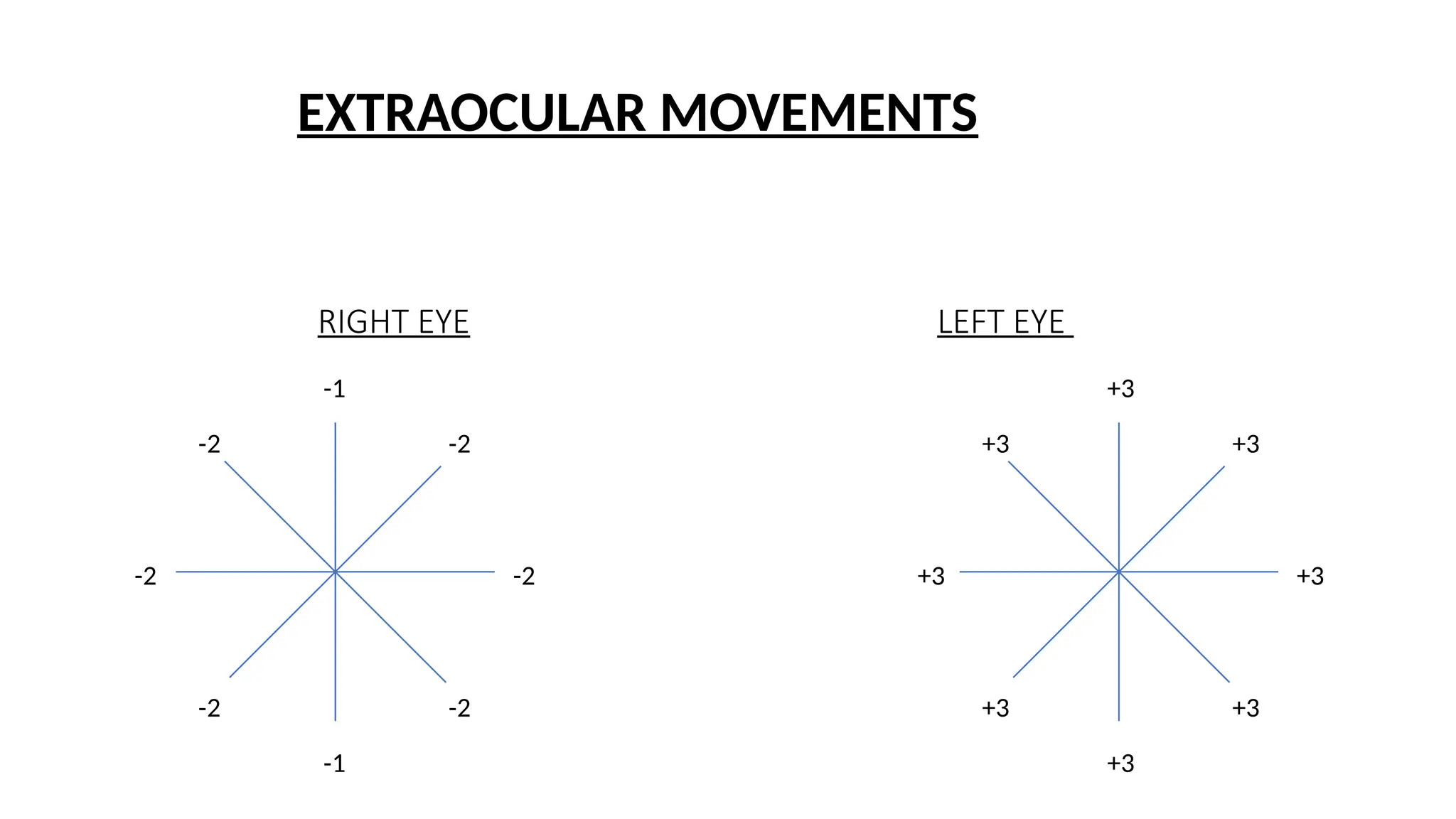
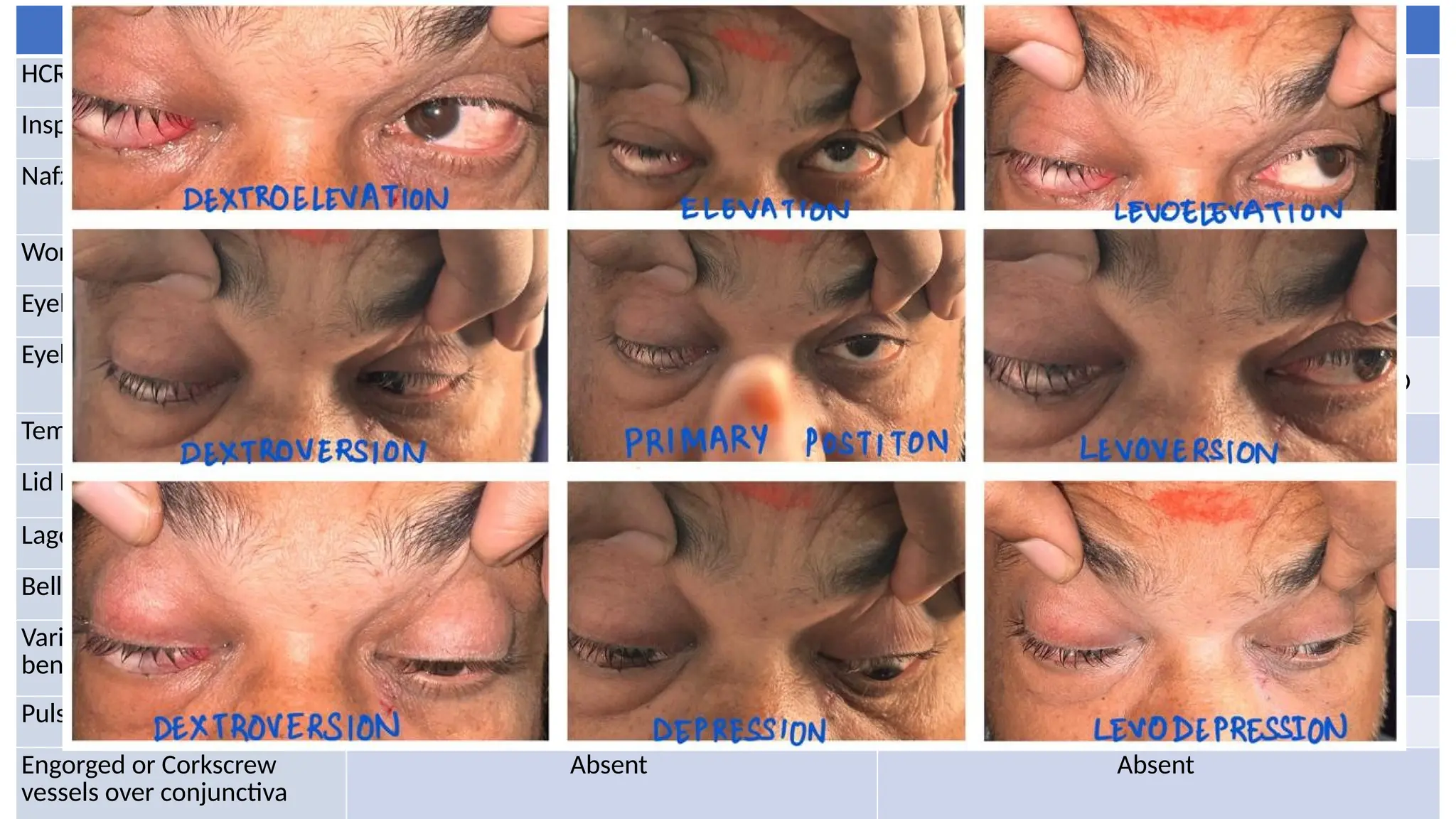
RE LE
HCRT 15degrees esotropia Central
Inspection Axial proptosis Axial proptosis
Nafziger’s Sign Negative (swollen eyelid visible beyond orbital
rim)
Negative
Worm’s Eye View Anteroposterior displacement of eyeball Anteroposterior displacement of eyeball
Eyebrows Normal Normal
Eyelids BE RETRACTED
BE UPPER AND LOWER LIDS FULLNESS NOTED
BE RETRACTED
BE UPPER AND LOWER LIDS FULLNESS NOTED
Temporal Flare Present Present
Lid Lag on Down Gaze Present Present
Lagophthalmos Present Present
Bell’s Phenomenon Good Good
Variation with valsalva or
bending forwards
Absent Absent
Pulsatile Proptosis No No
Engorged or Corkscrew
vessels over conjunctiva
Absent Absent
15.
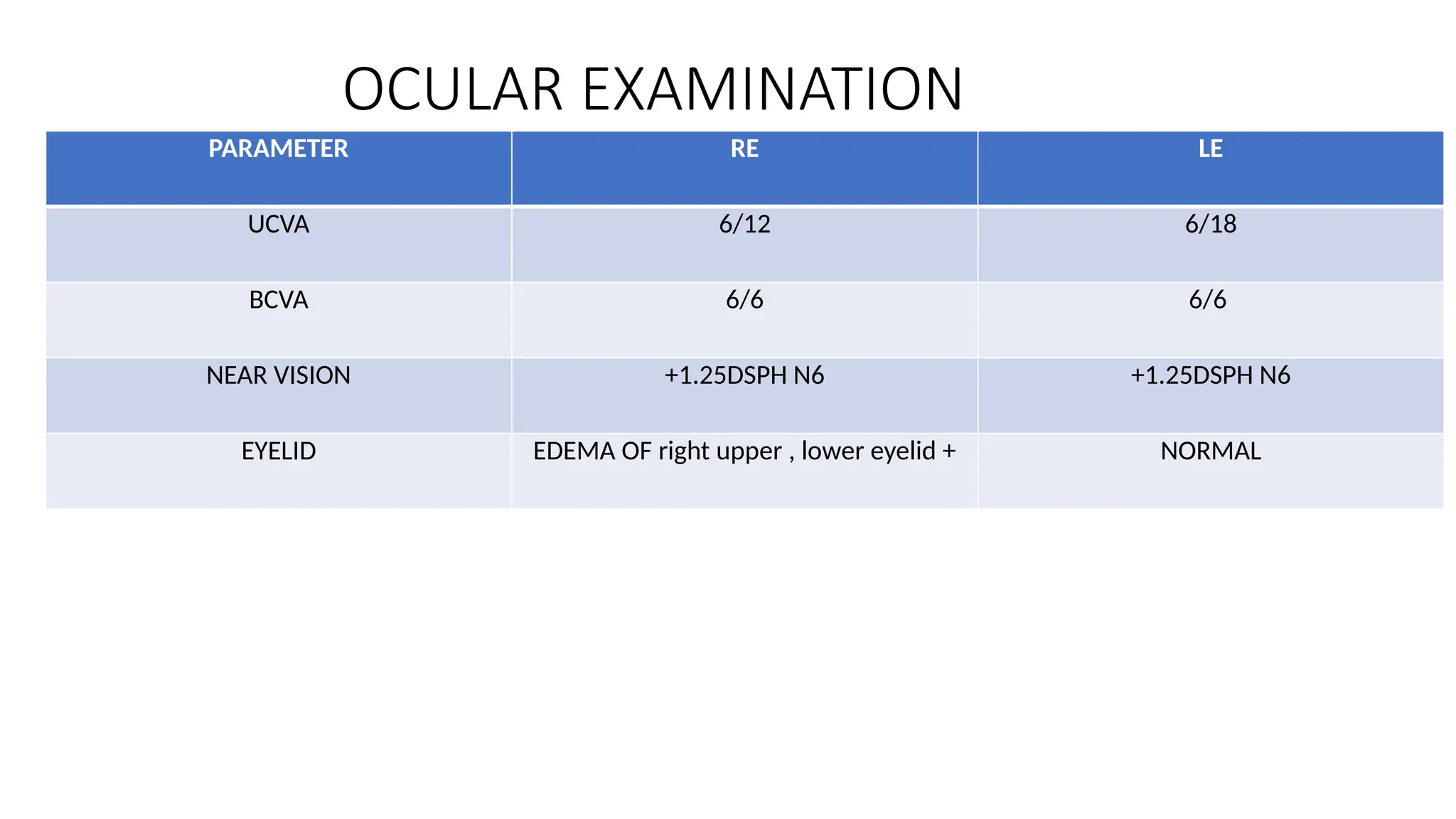
OCULAR EXAMINATION
PARAMETER RELE
UCVA 6/12 6/18
BCVA 6/6 6/6
NEAR VISION +1.25DSPH N6 +1.25DSPH N6
EYELID EDEMA OF right upper , lower eyelid + NORMAL
16.
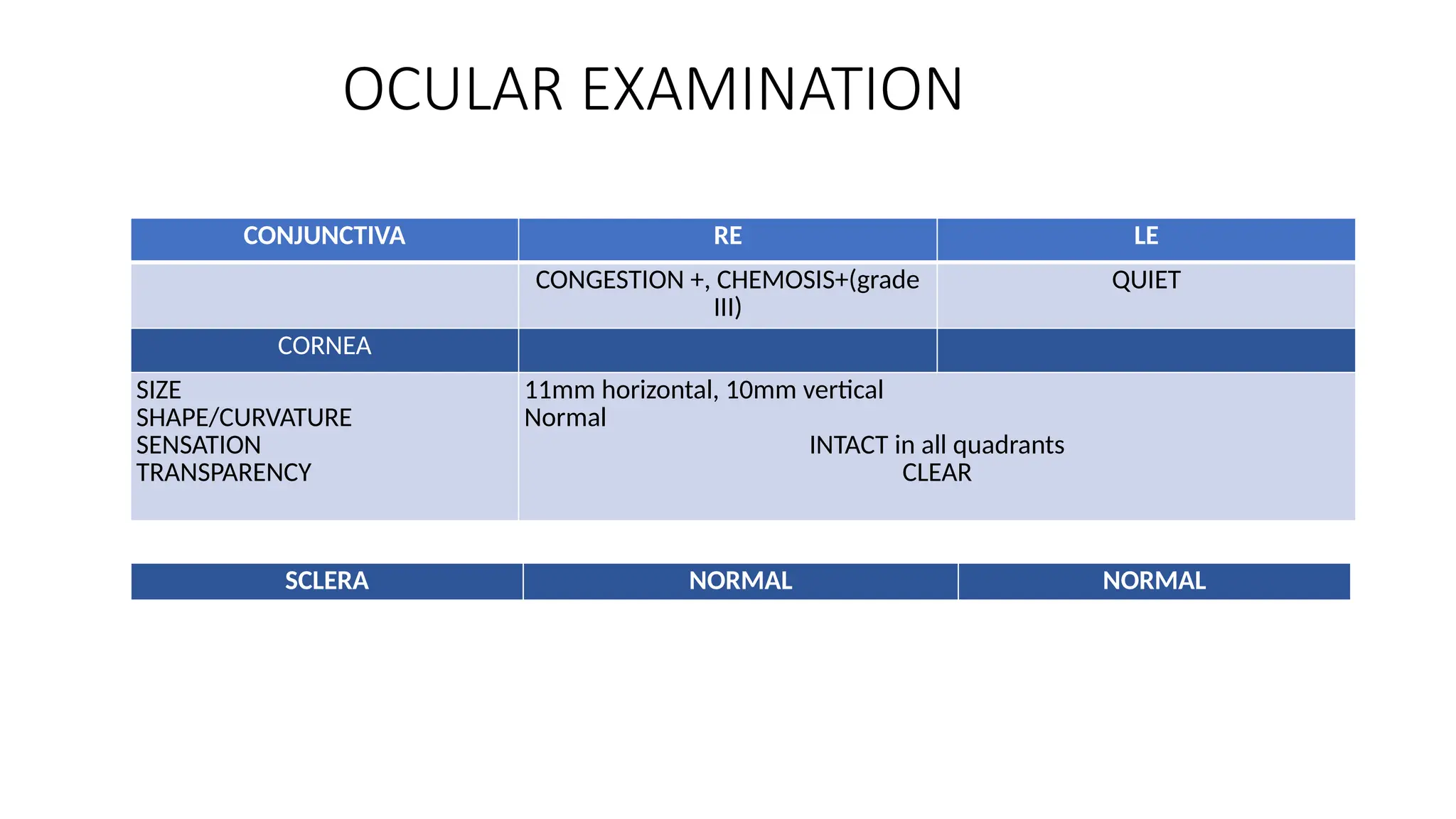
CONJUNCTIVA RE LE
CONGESTION+, CHEMOSIS+(grade
III)
QUIET
CORNEA
SIZE
SHAPE/CURVATURE
SENSATION
TRANSPARENCY
11mm horizontal, 10mm vertical
Normal
INTACT in all quadrants
CLEAR
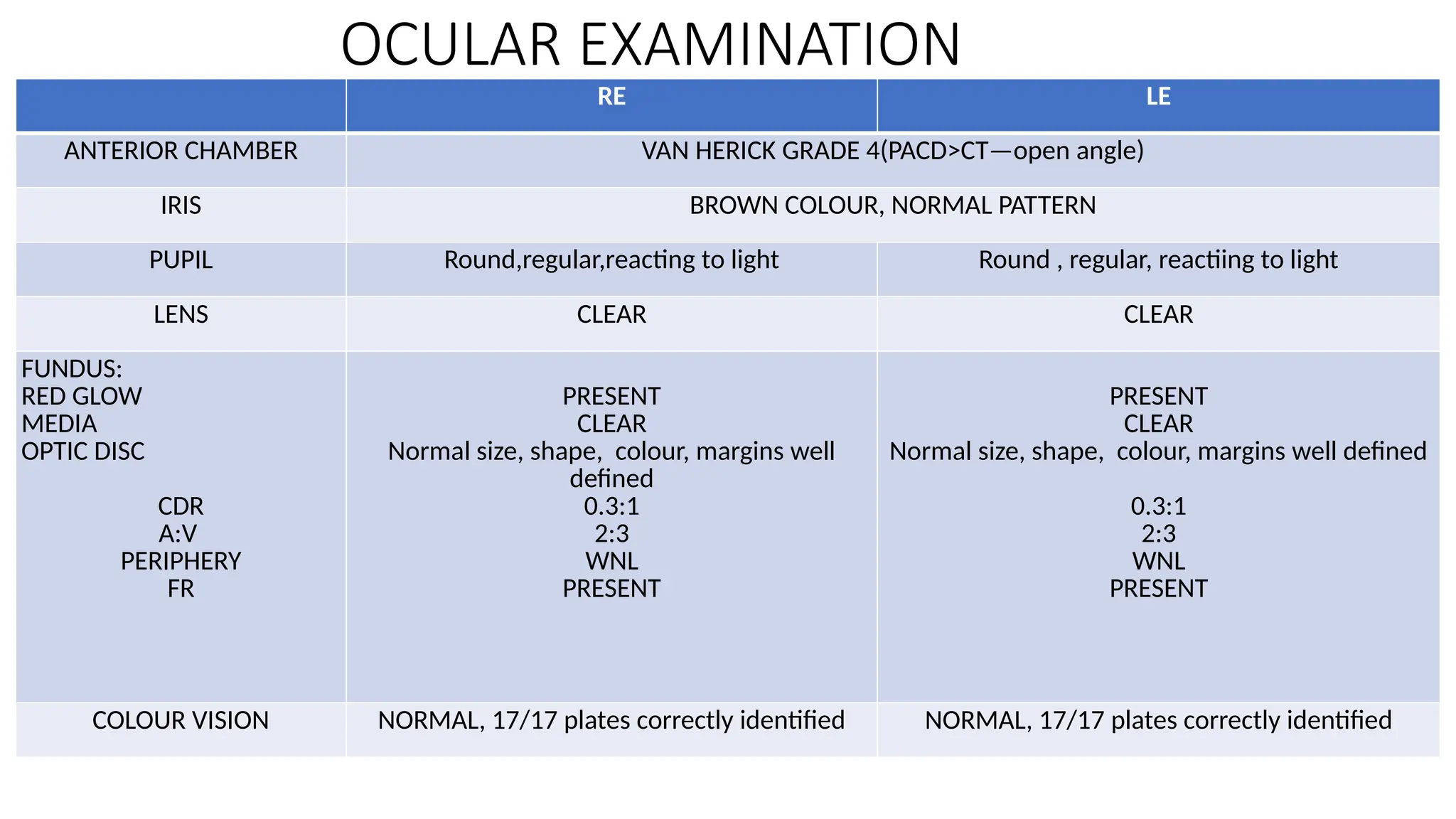
OCULAR EXAMINATION
SCLERA NORMAL NORMAL
17.
RE LE
ANTERIOR CHAMBERVAN HERICK GRADE 4(PACD>CT—open angle)
IRIS BROWN COLOUR, NORMAL PATTERN
PUPIL Round,regular,reacting to light Round , regular, reactiing to light
LENS CLEAR CLEAR
FUNDUS:
RED GLOW
MEDIA
OPTIC DISC
CDR
A:V
PERIPHERY
FR
PRESENT
CLEAR
Normal size, shape, colour, margins well
defined
0.3:1
2:3
WNL
PRESENT
PRESENT
CLEAR
Normal size, shape, colour, margins well defined
0.3:1
2:3
WNL
PRESENT
COLOUR VISION NORMAL, 17/17 plates correctly identified NORMAL, 17/17 plates correctly identified
OCULAR EXAMINATION
18.
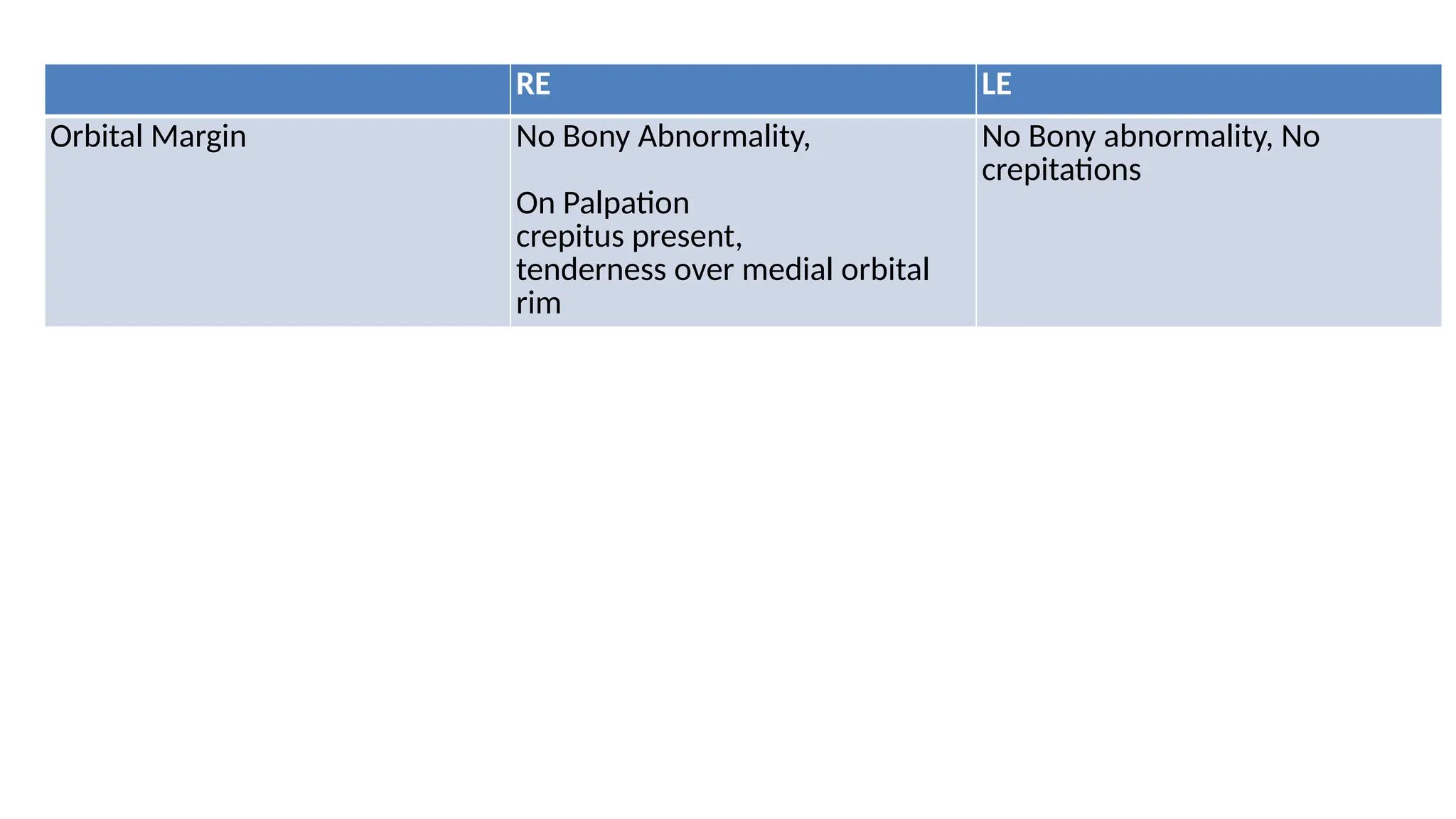
RE LE
Orbital MarginNo Bony Abnormality,
On Palpation
crepitus present,
tenderness over medial orbital
rim
No Bony abnormality, No
crepitations
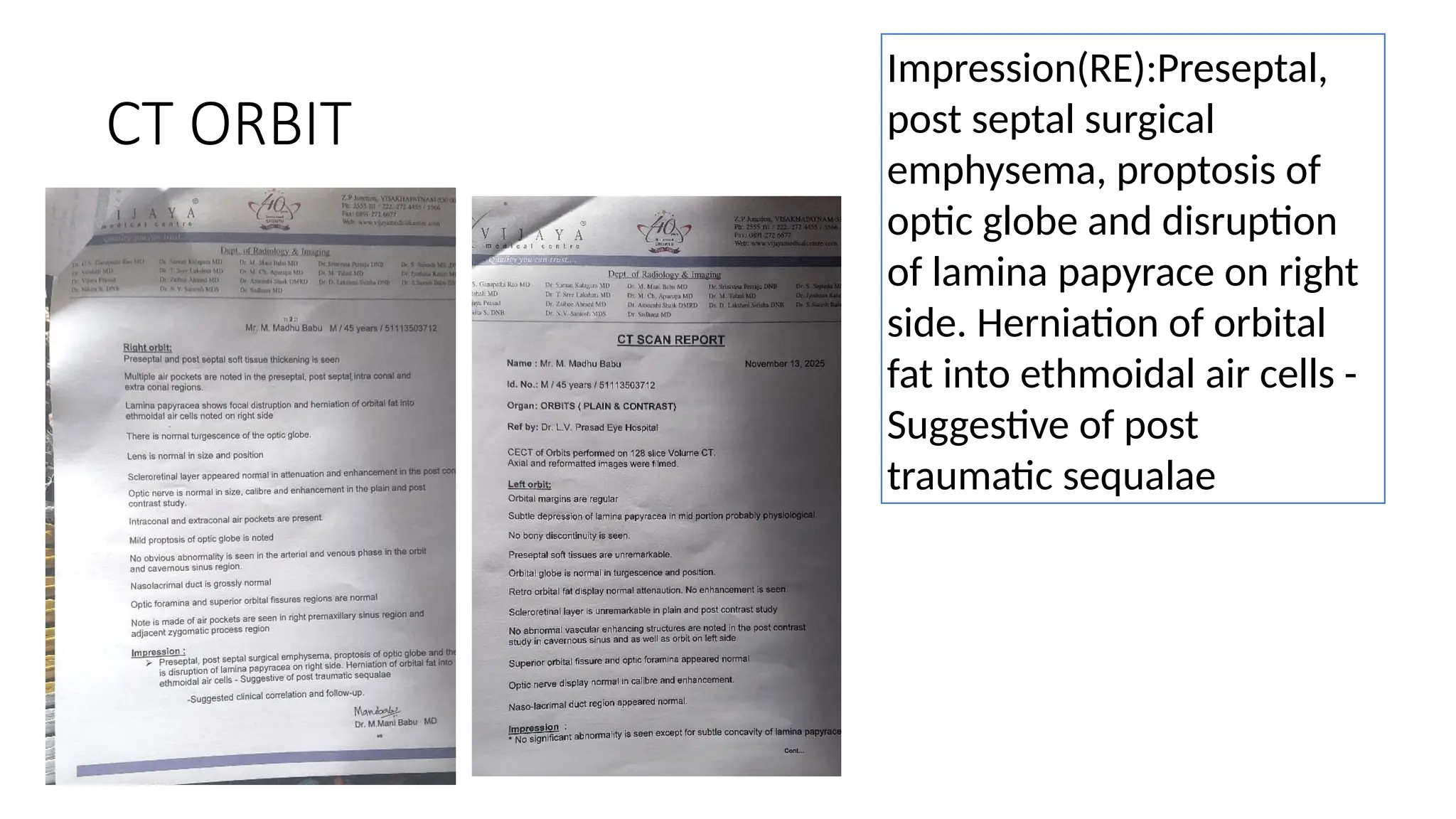
CT ORBIT
Impression(RE):Preseptal,
post septalsurgical
emphysema, proptosis of
optic globe and disruption
of lamina papyrace on right
side. Herniation of orbital
fat into ethmoidal air cells -
Suggestive of post
traumatic sequalae
23.
TREATMENT
• Cold compressestwice a day
• Avoid nose blowing,straining ,coughing
• Tab DICLOFENAC SODIUM 50mg BD PO for 5days
• Tab CEFEXIME 200mg BD PO for 5days
• Tab LEVOCETRIZINE 10mg HS for 3 days
• REASURRANCE OF THE PATIENT
• REGULAR FOLLOW UP