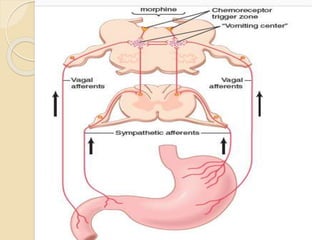
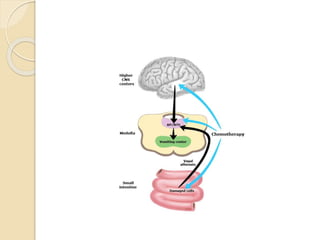
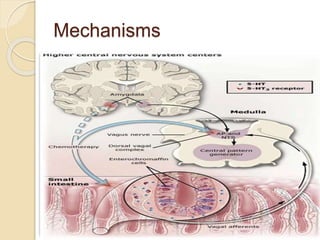
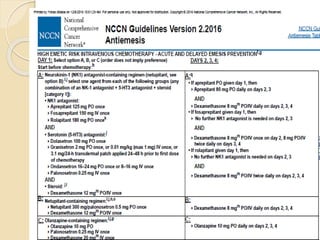
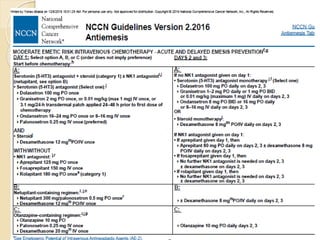
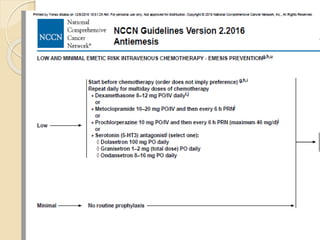
This document outlines chemotherapy-induced nausea and vomiting (CINV), including its types, pathophysiology, predictive factors, and prevention/treatment approaches. There are three types of CINV - acute, delayed, and anticipatory. The pathophysiology involves the central nervous system and neurotransmitters like dopamine, serotonin, and substance P. Predictive factors include the chemotherapy agent/dose, patient characteristics, and antiemetic regimen. Prevention/treatment involves 5-HT3 receptor antagonists, neurokinin-1 receptor antagonists, glucocorticoids, and dopamine receptor antagonists. Combination therapy is most effective at preventing both acute and delayed CINV.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









