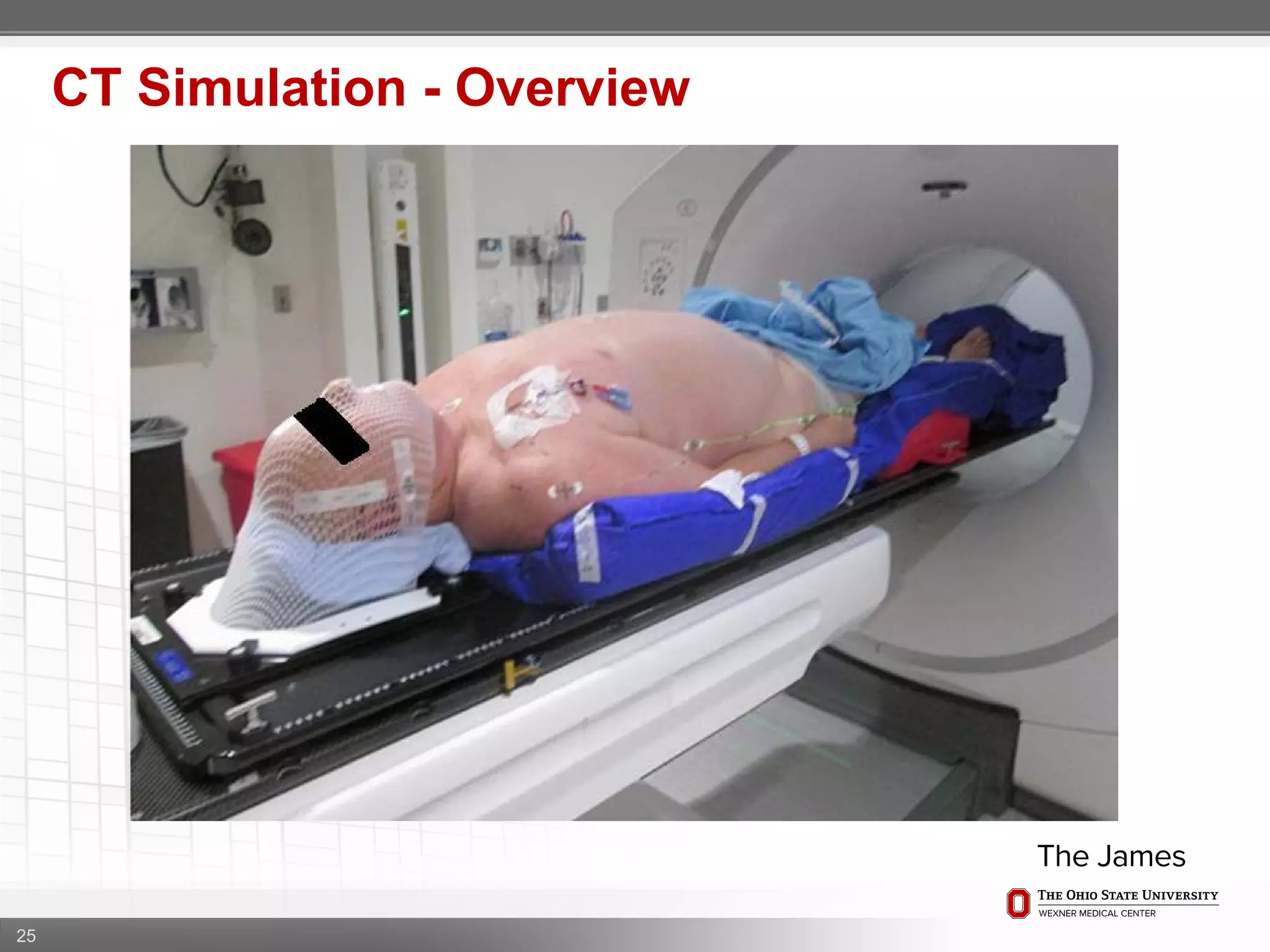
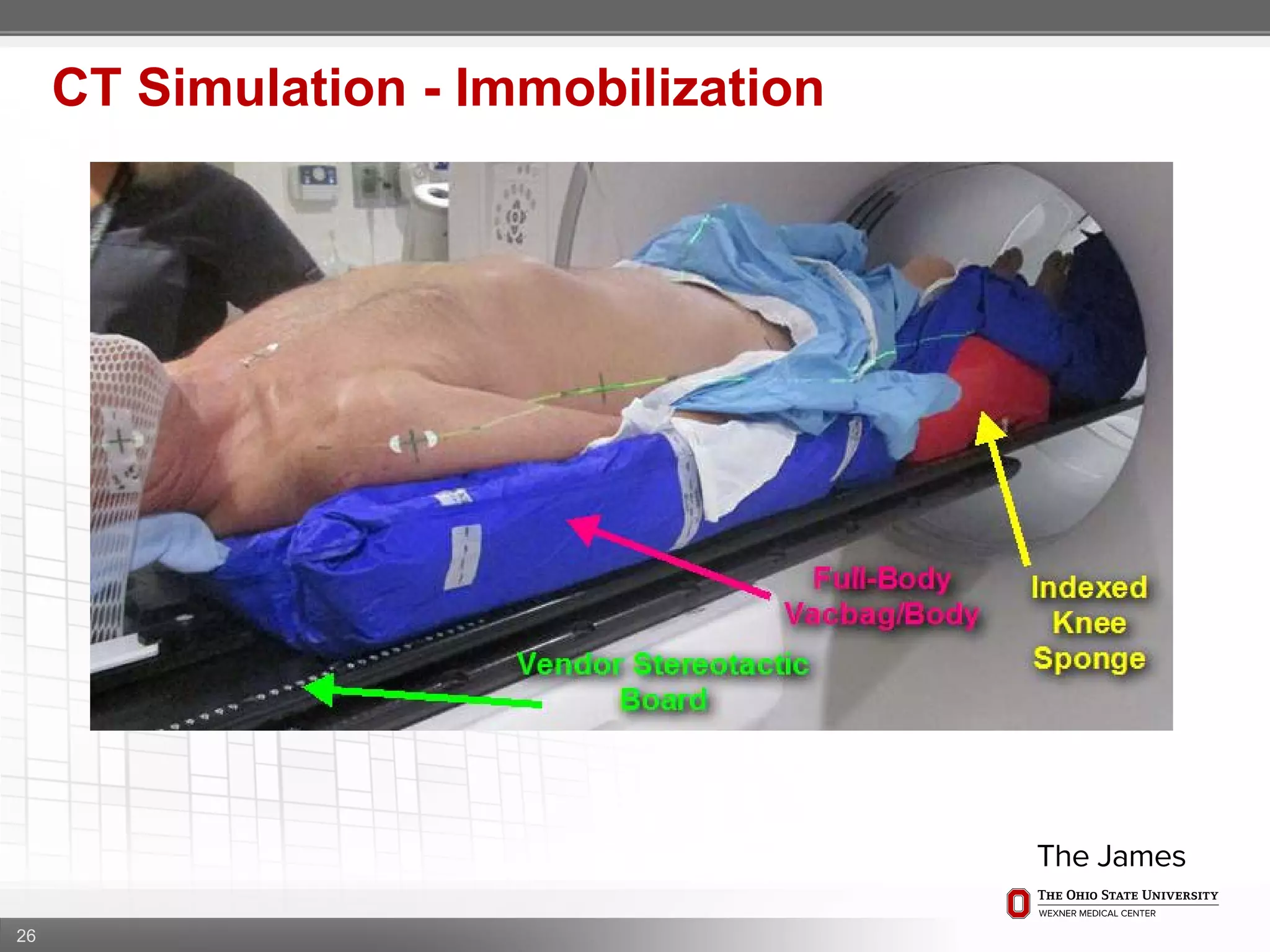
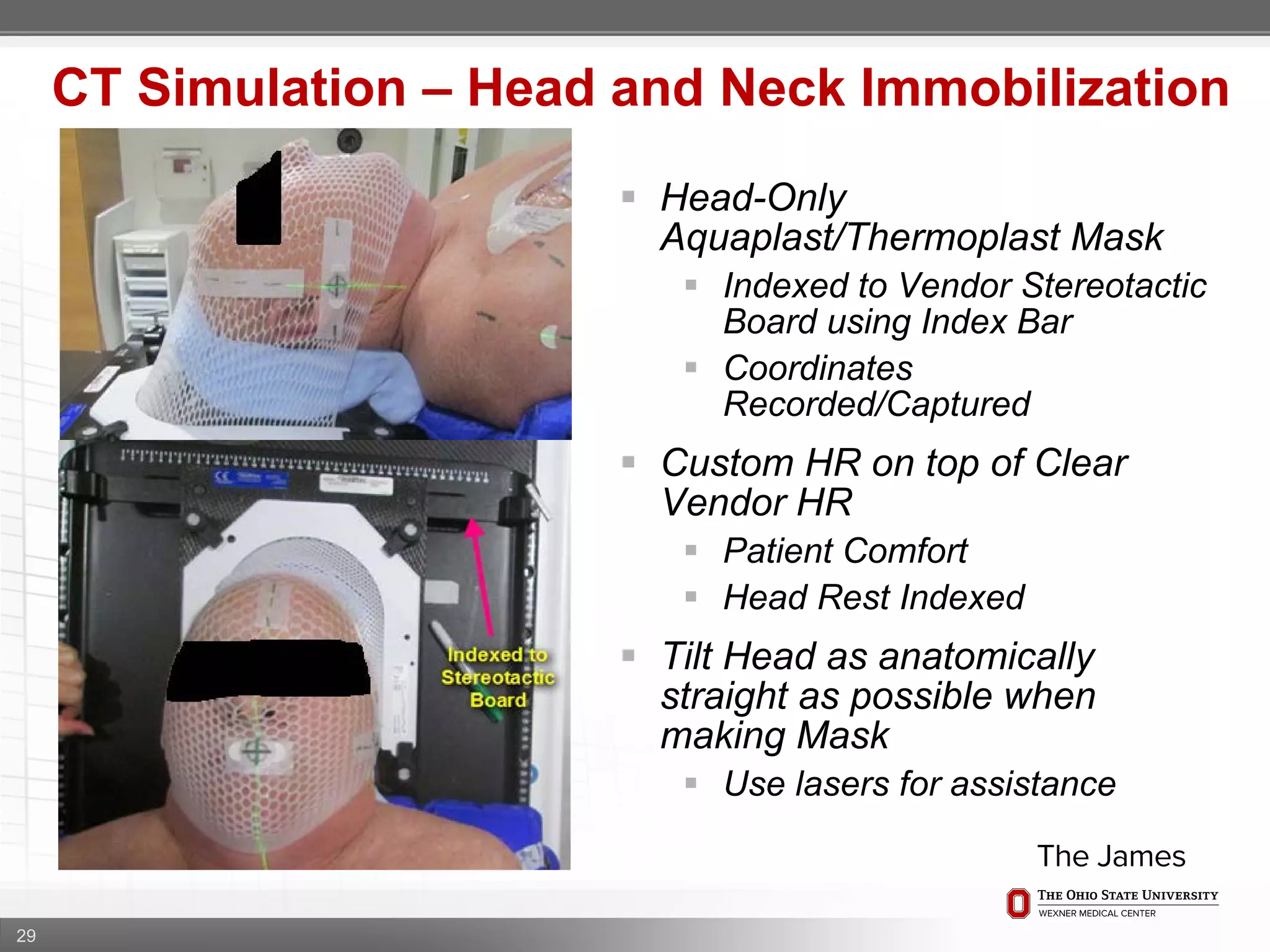
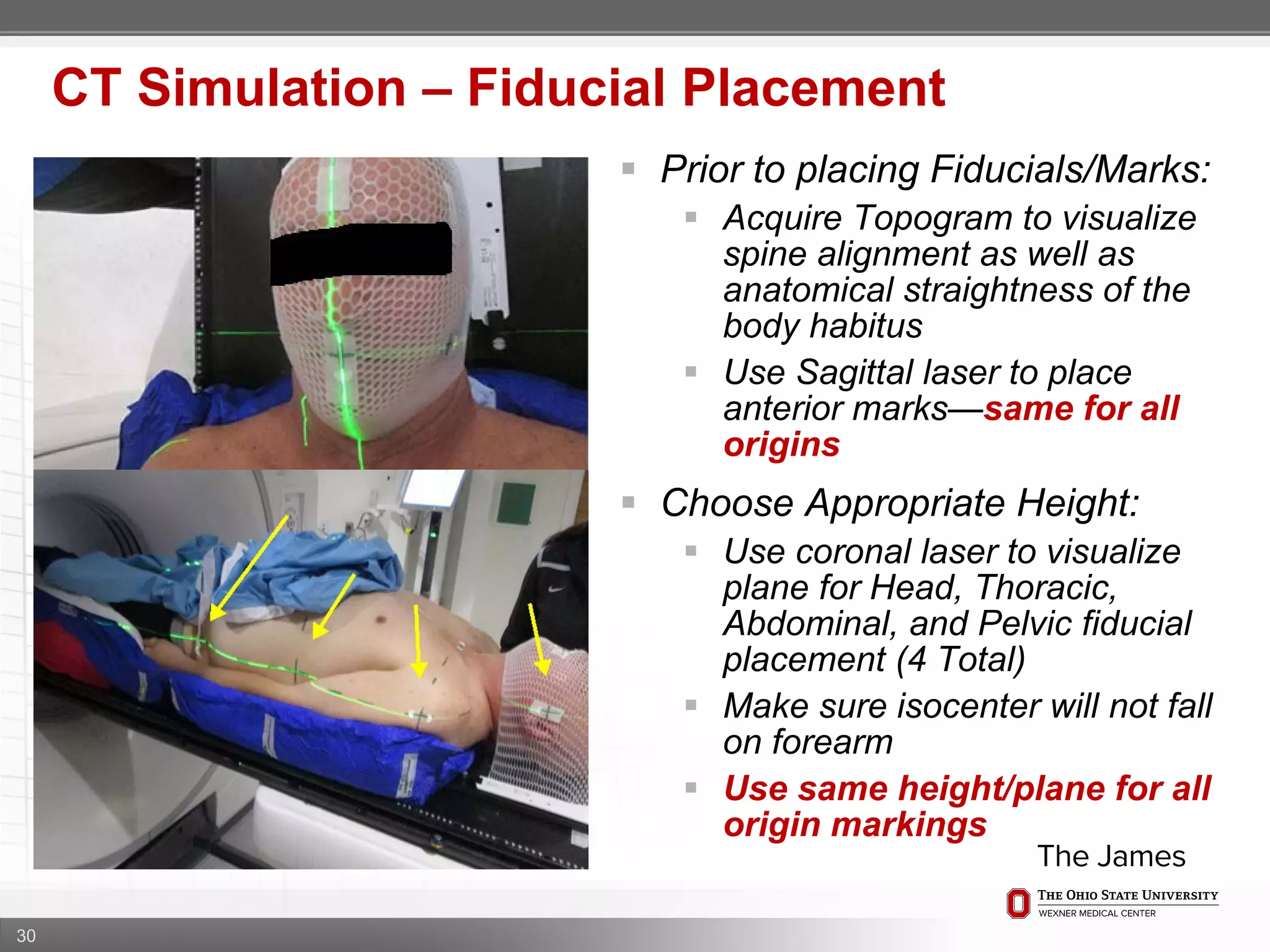
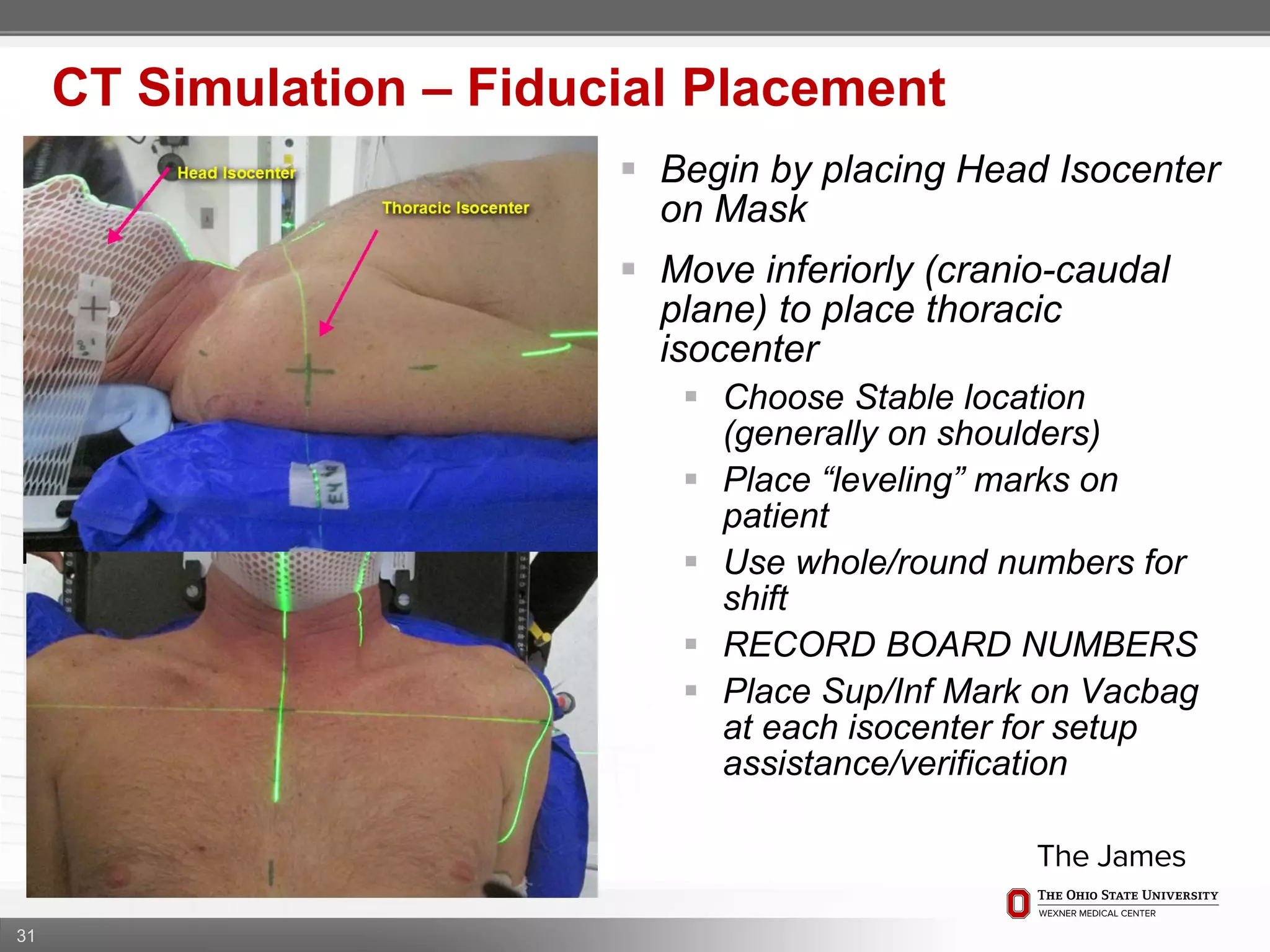
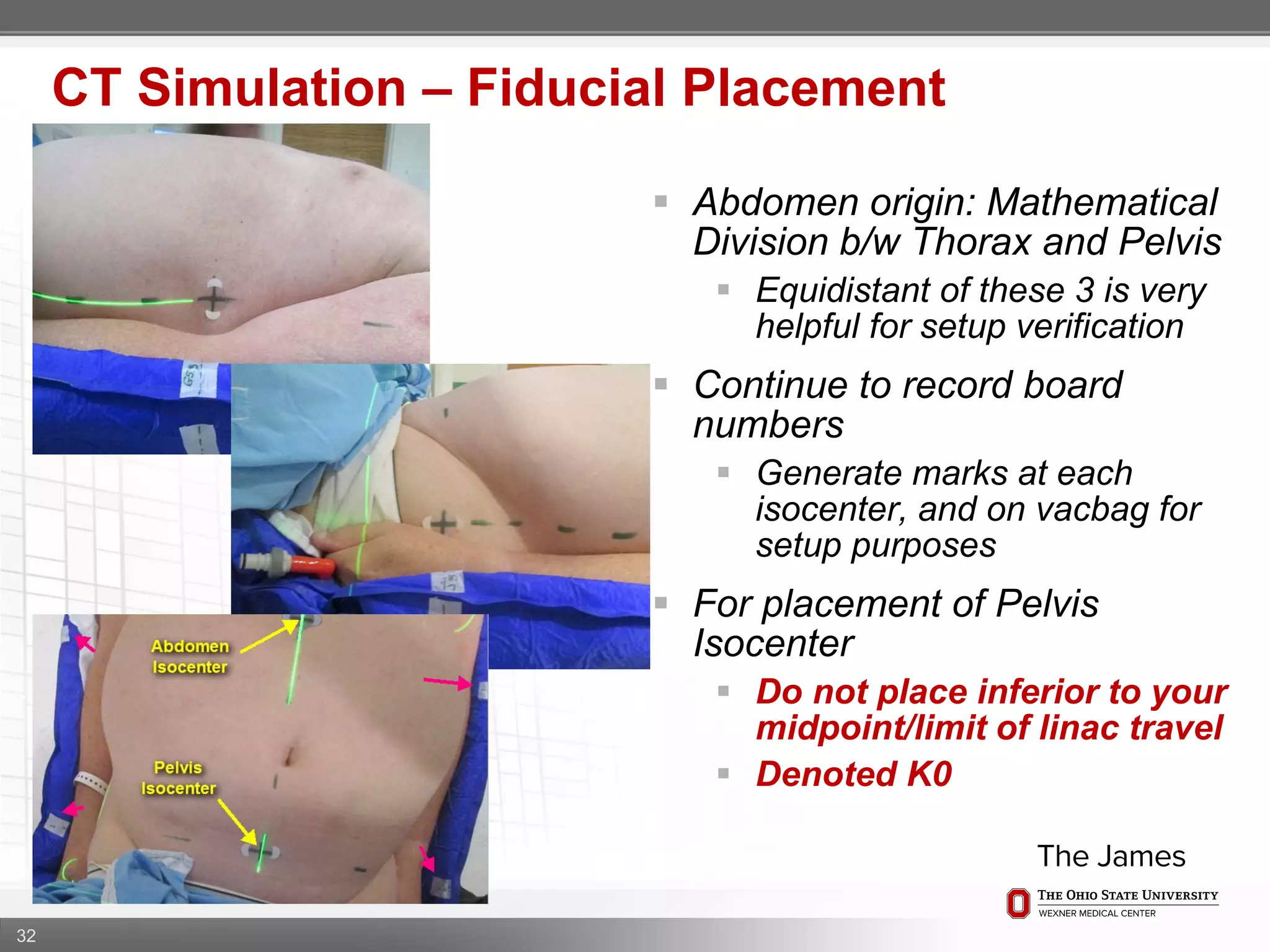
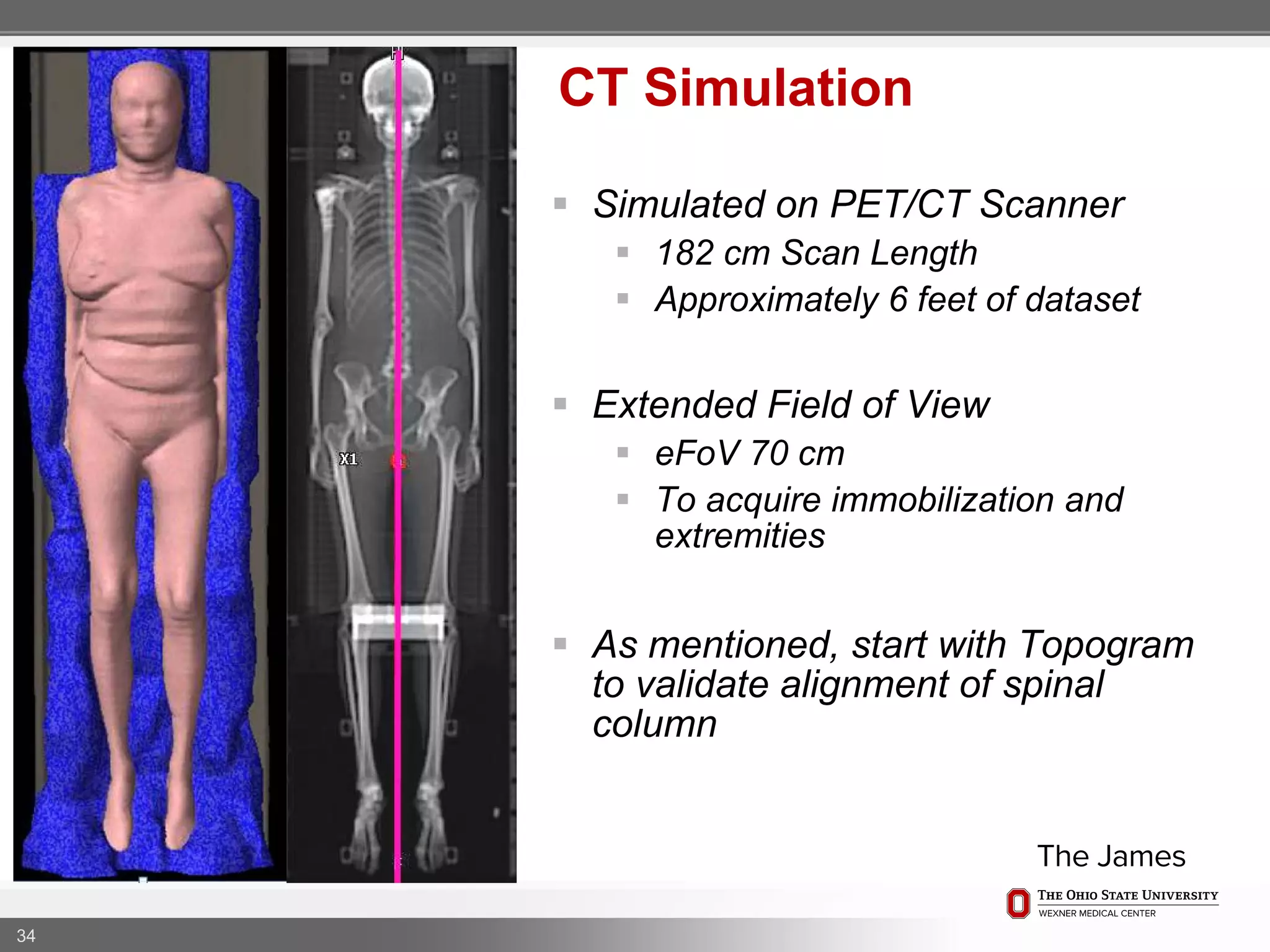
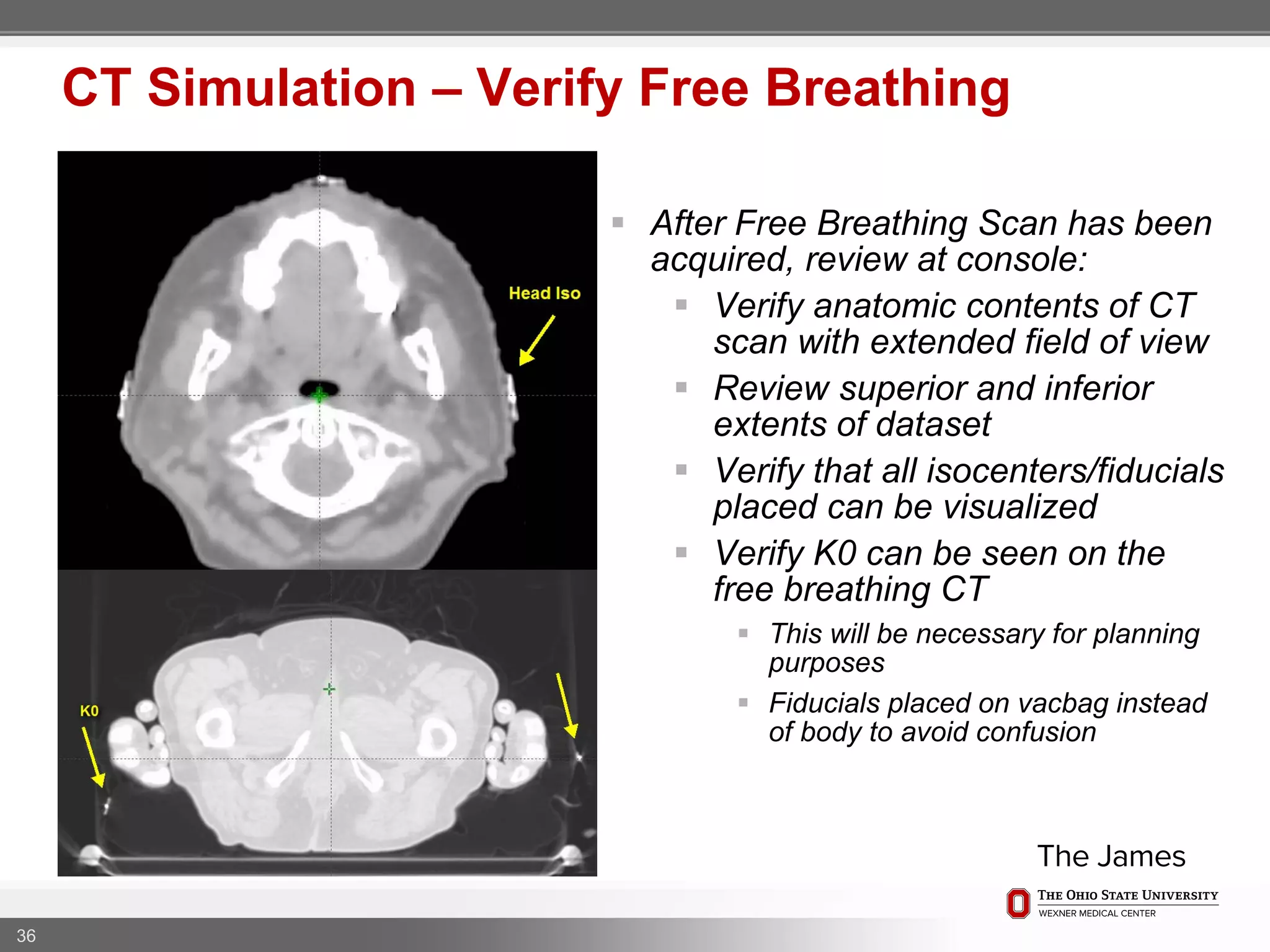
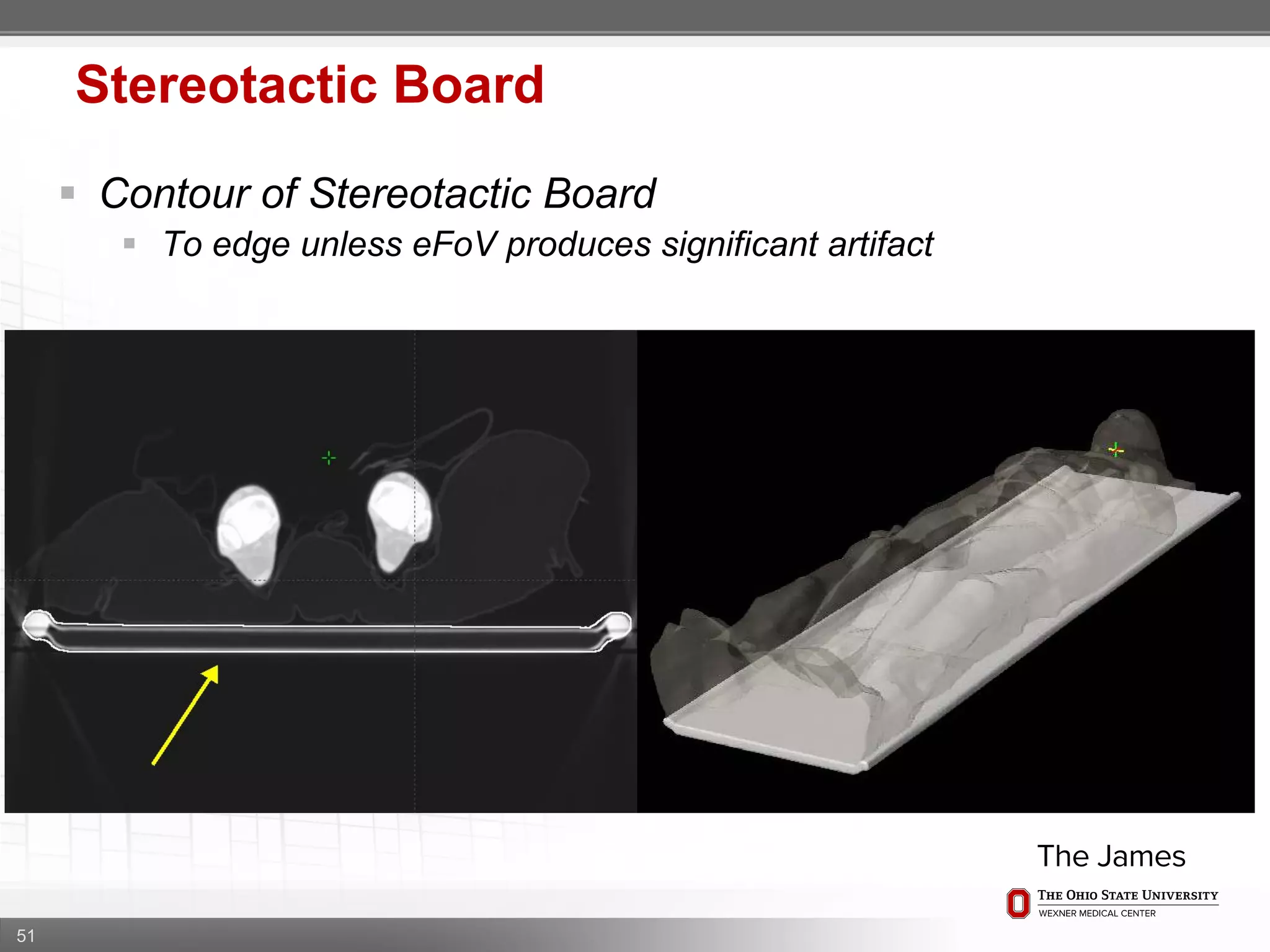
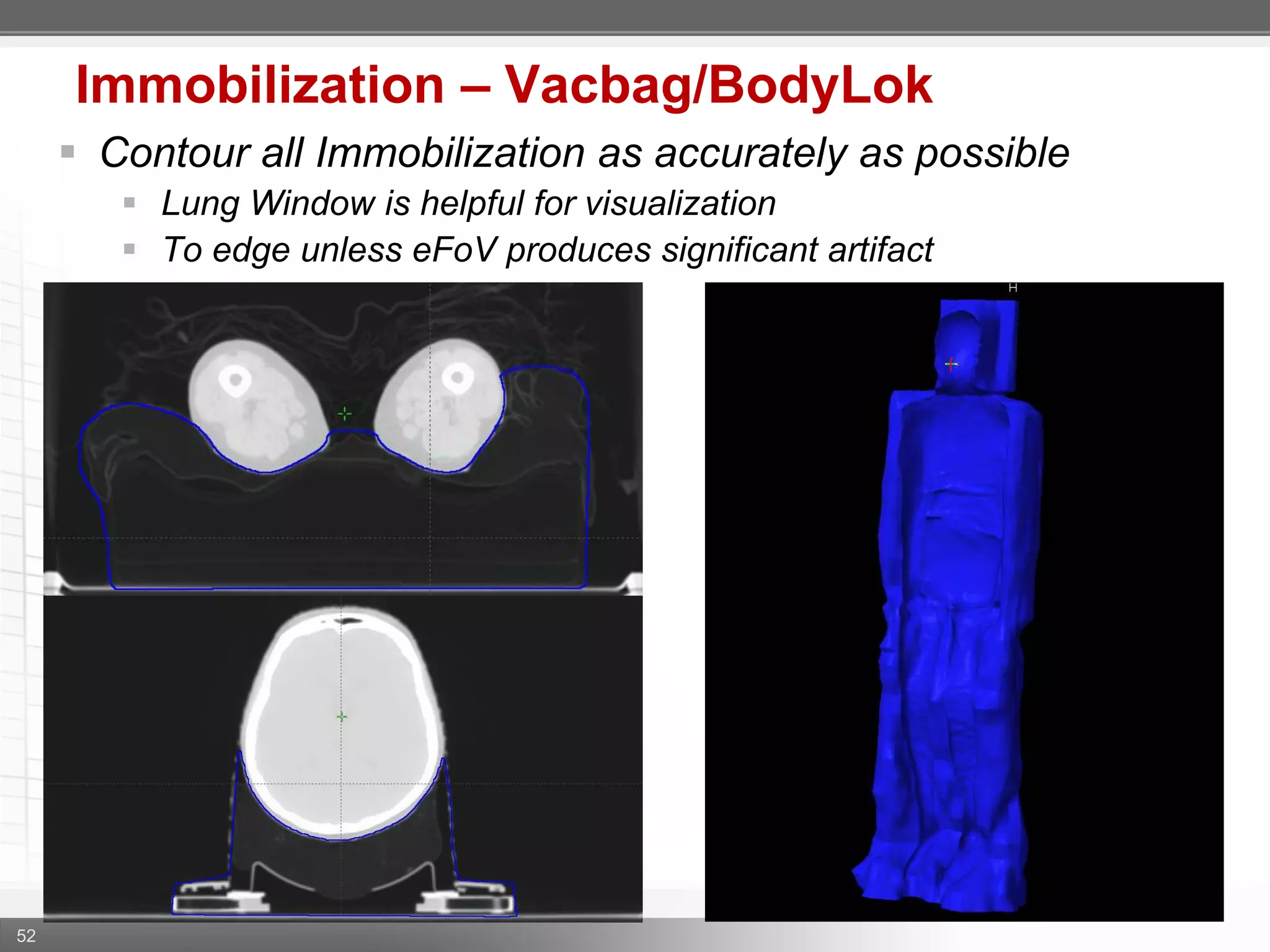
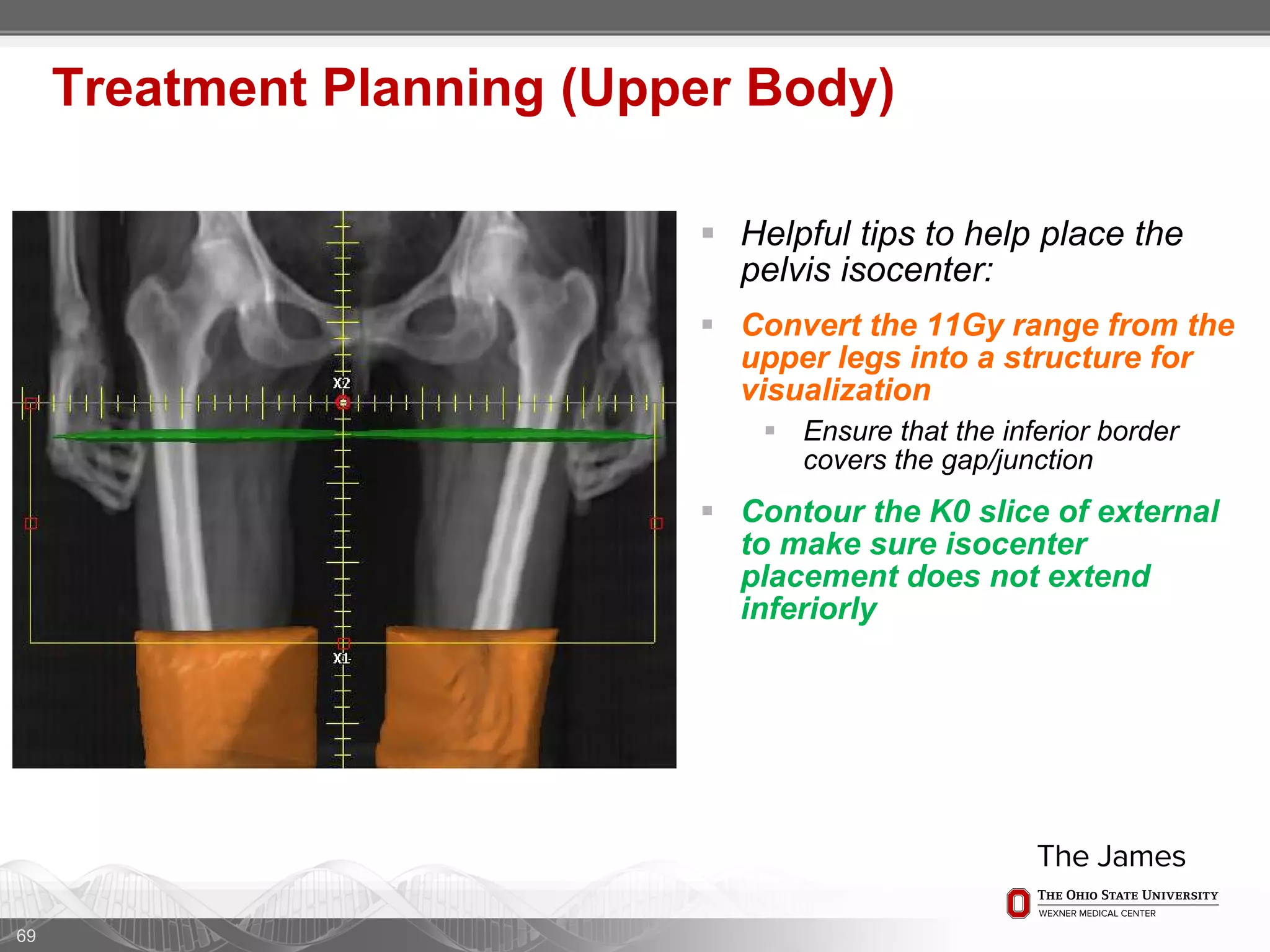
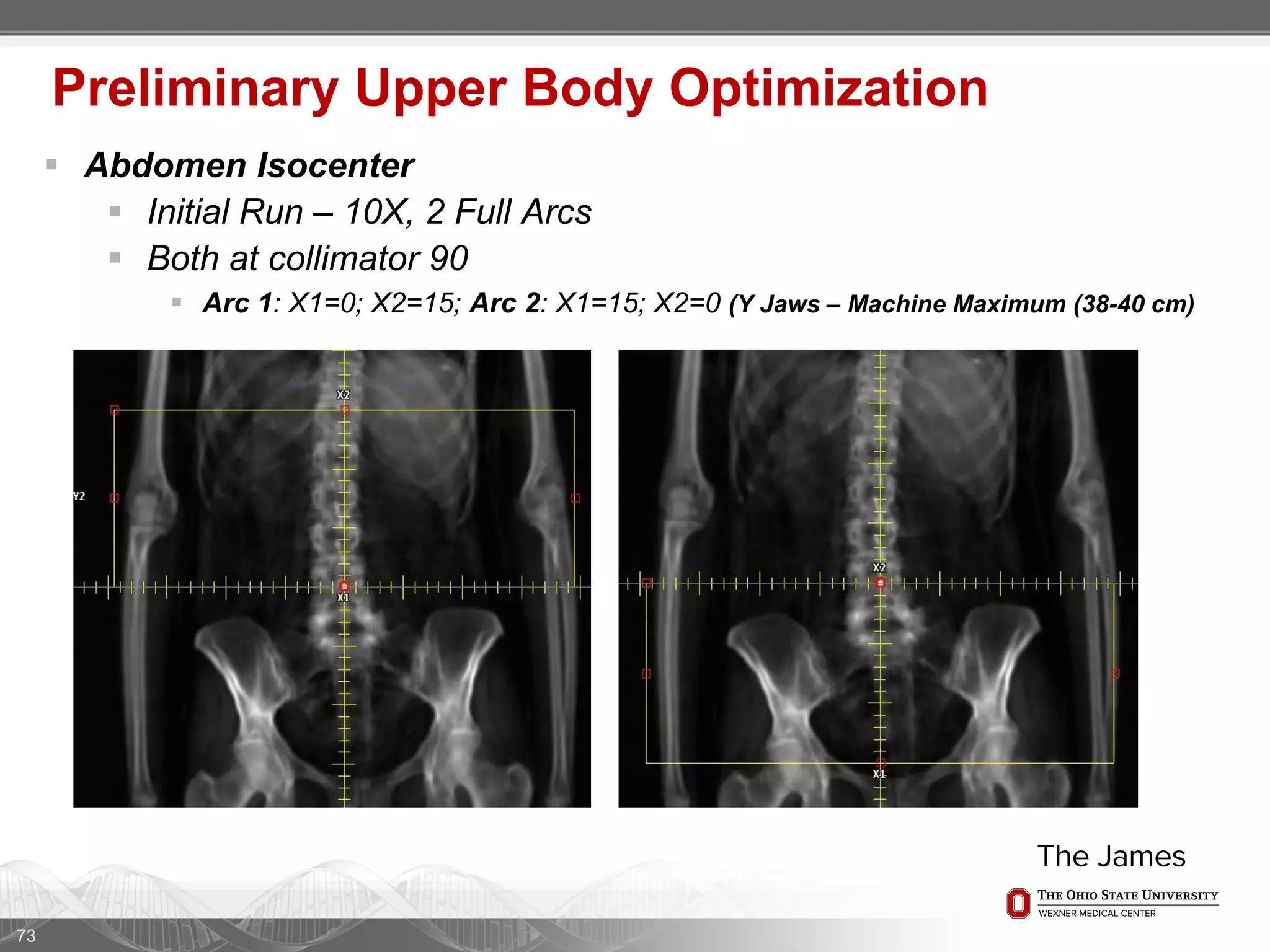
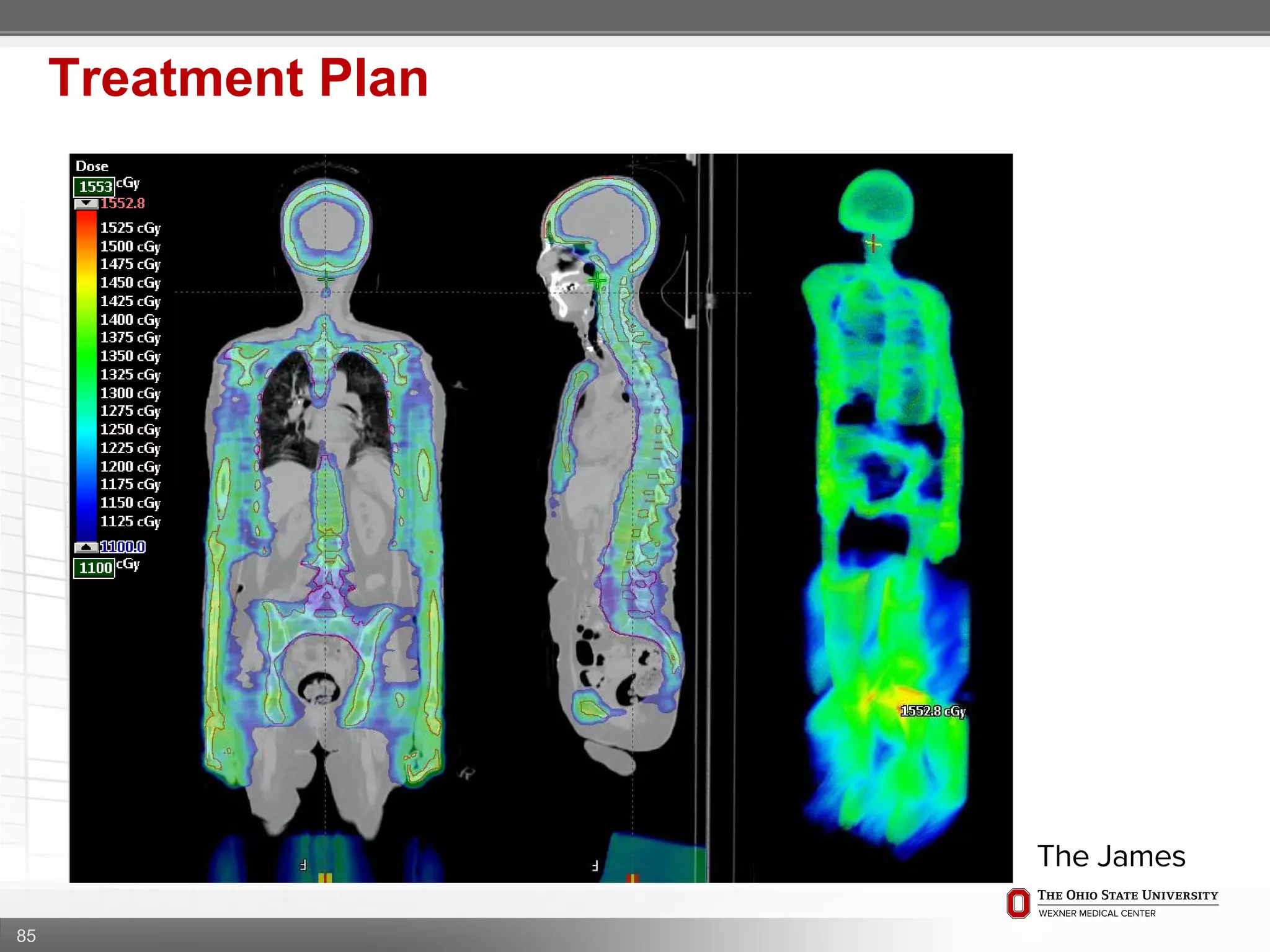
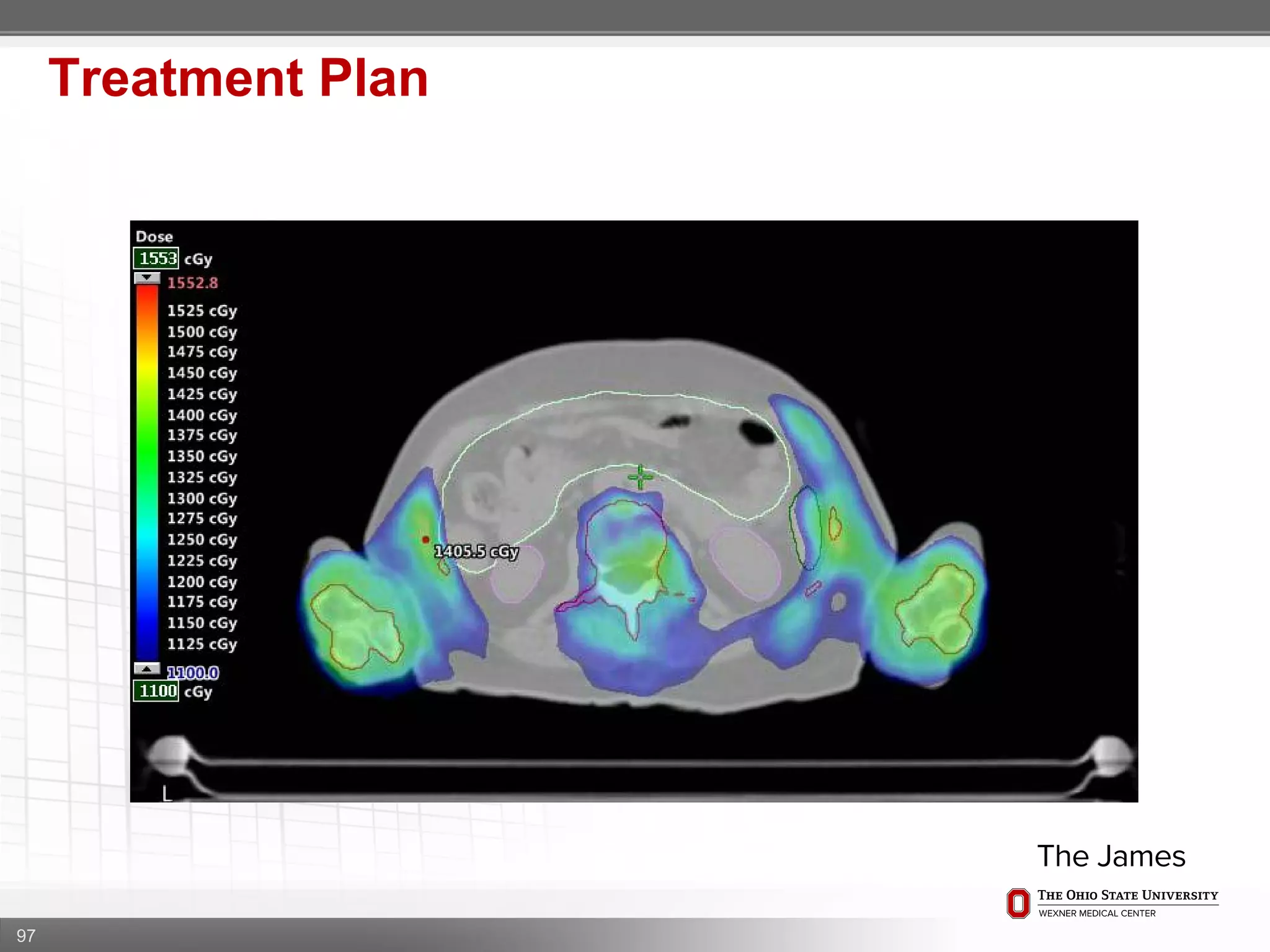
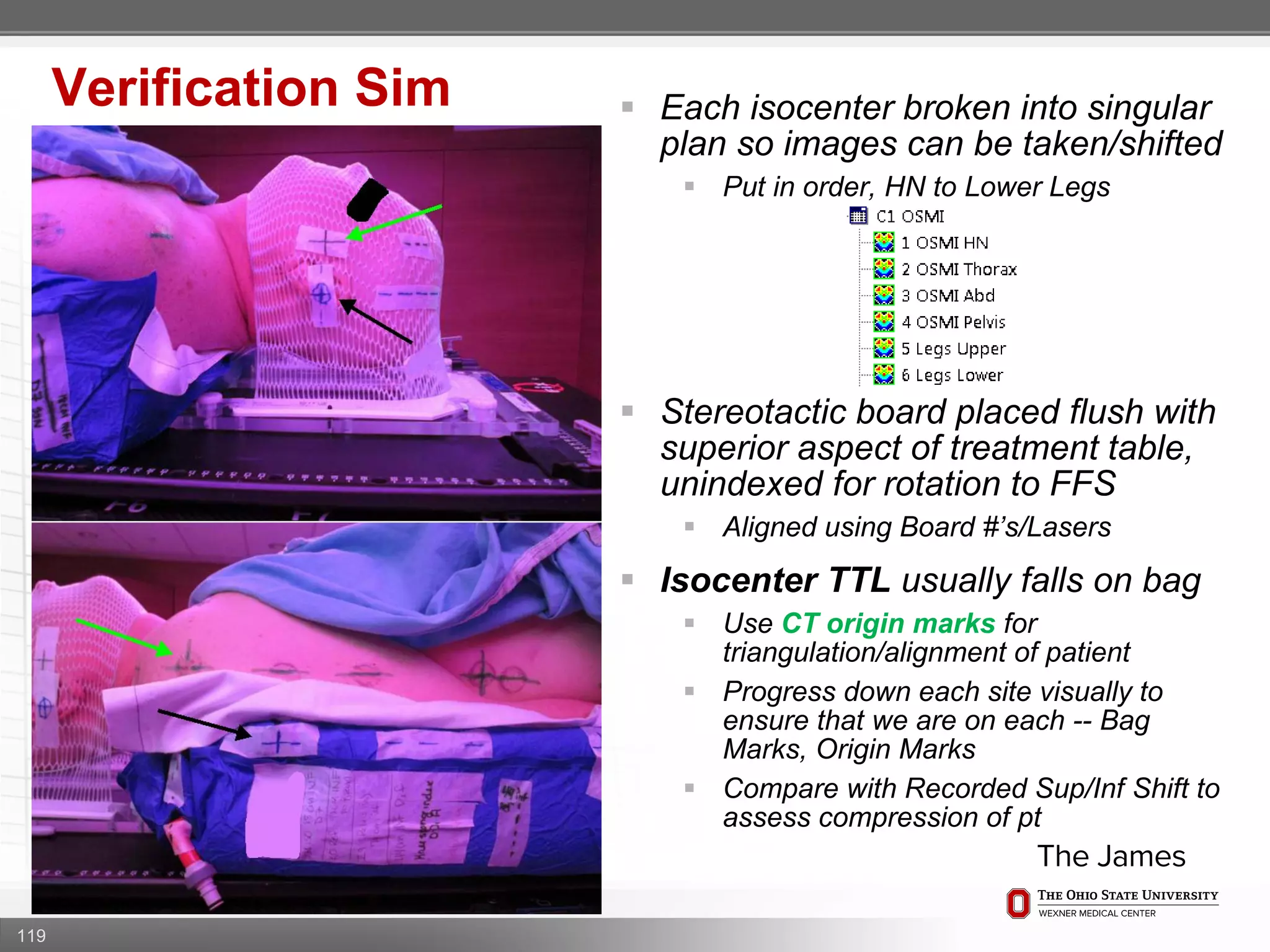
1. CT simulation involves immobilizing the patient in a vacbag on a stereotactic board with a custom headrest and mask for head and neck immobilization. Fiducial markers are placed at the head, thorax, abdomen, and pelvis to aid in daily setup verification.
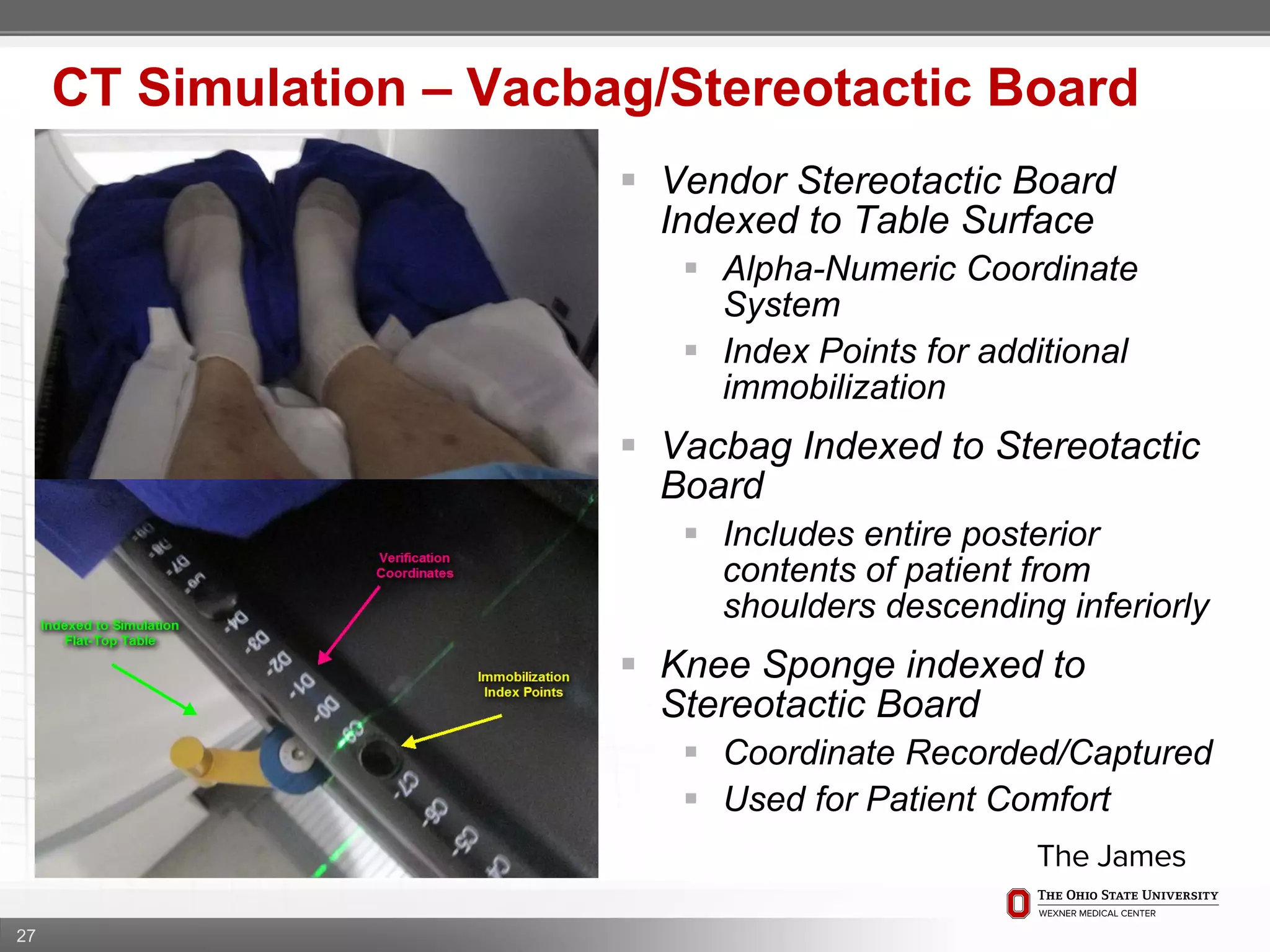
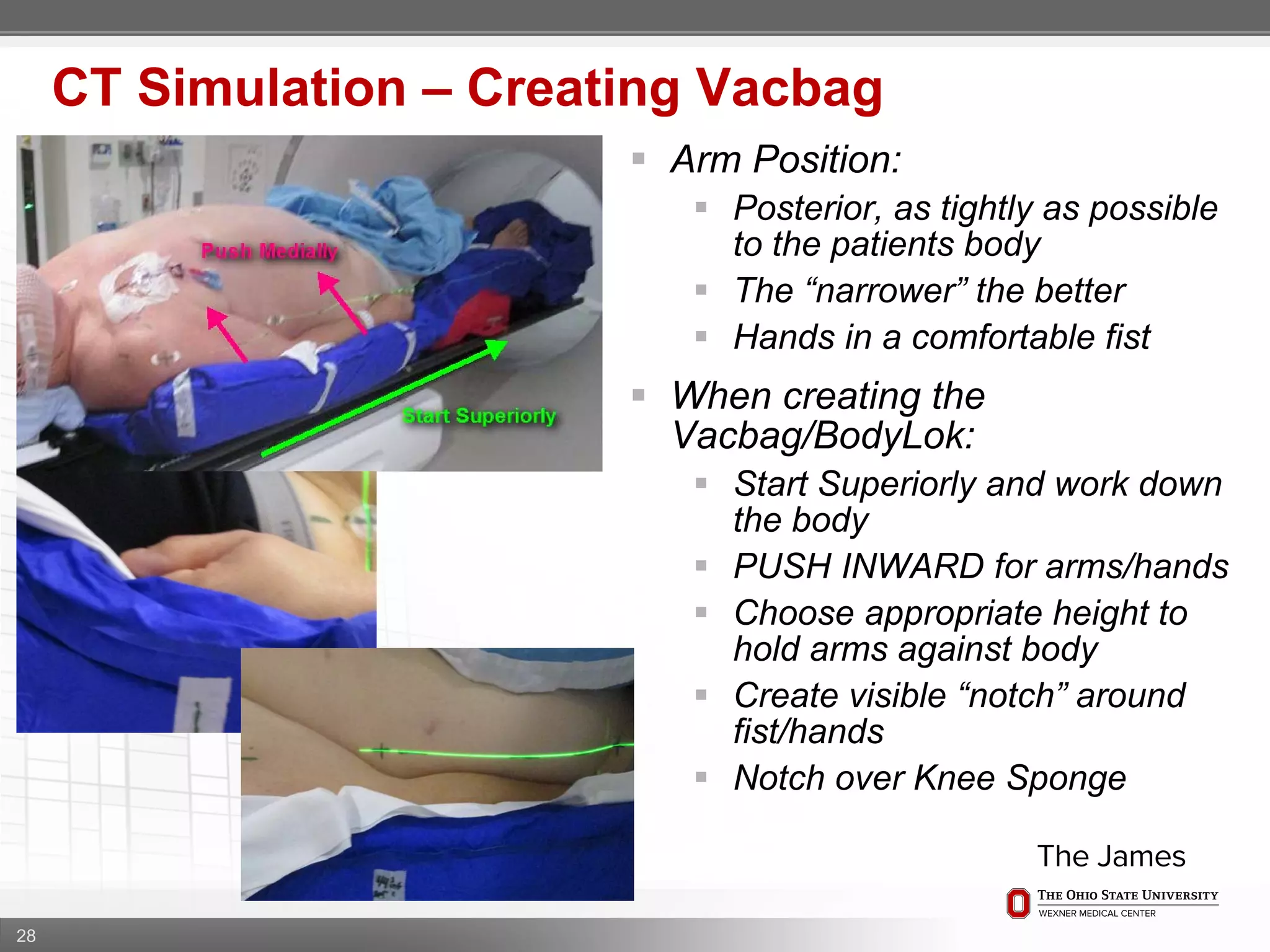
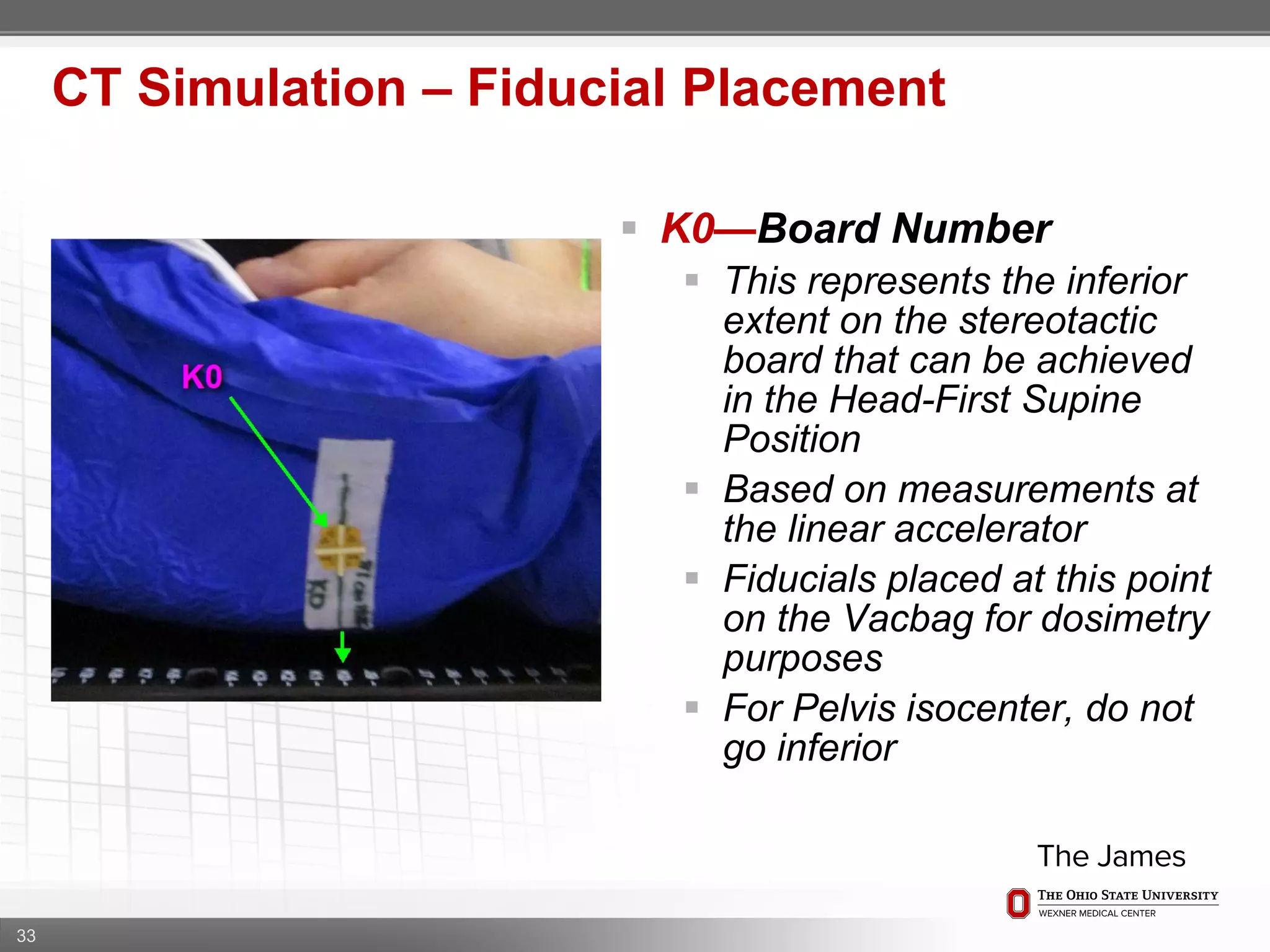
2. Care is taken to push the arms tightly against the body when creating the vacbag and to index all immobilization devices to the stereotactic board for reproducibility. Fiducials are placed at standardized coronal planes and levels are marked on the vacbag to guide setup.
3. The goal is to immobilize the patient and place reproducible fiducial markers to allow for precise targeting of the marrow and sparing