This document provides information on newborn assessment including:
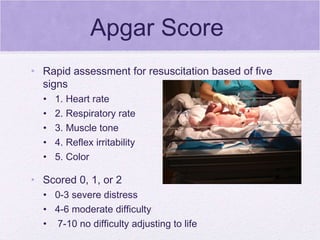
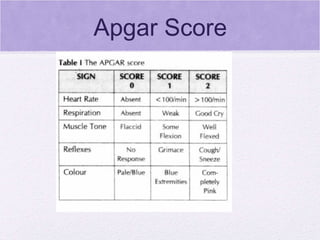
1) Describing the Apgar score system used to evaluate a newborn's health after delivery.
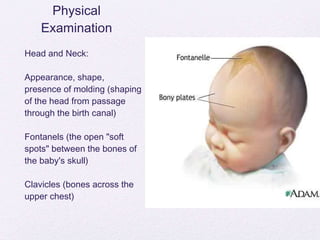
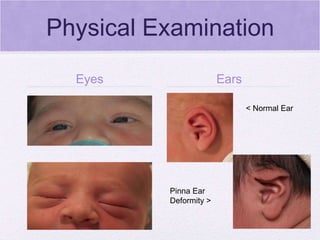
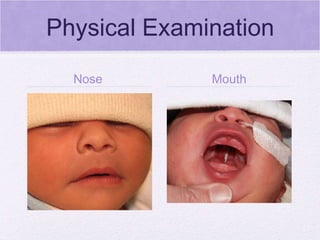
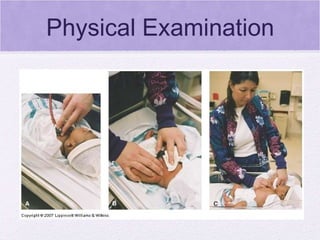
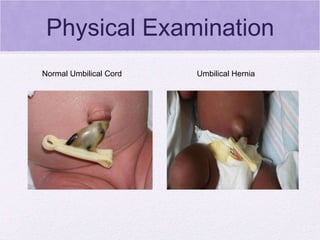
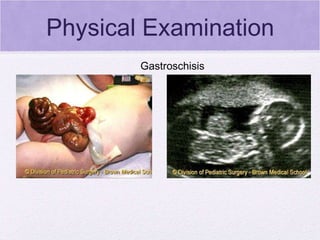
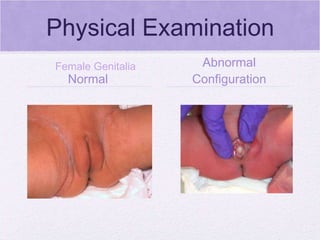
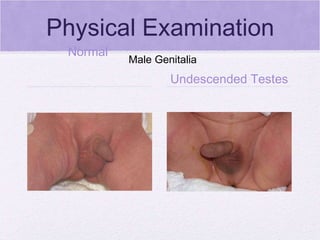
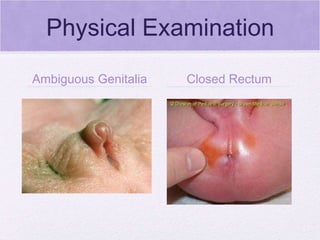
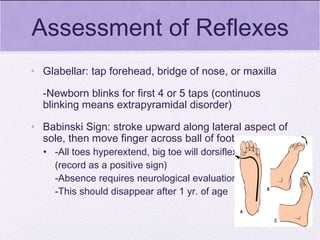
2) Outlining the steps of the physical examination of a newborn including assessment of vital signs, skin, head, chest, heart, abdomen, extremities and genitals.
3) Detailing the measurements taken of a newborn including weight, length, head circumference and gestational age assessment.