This document discusses peripheral neuropathy and provides details on various types including:
- Peripheral neuropathy can affect nerves in the arms, legs, or other areas and be classified by pathology, size of nerves affected, or function (sensory, motor, autonomic).
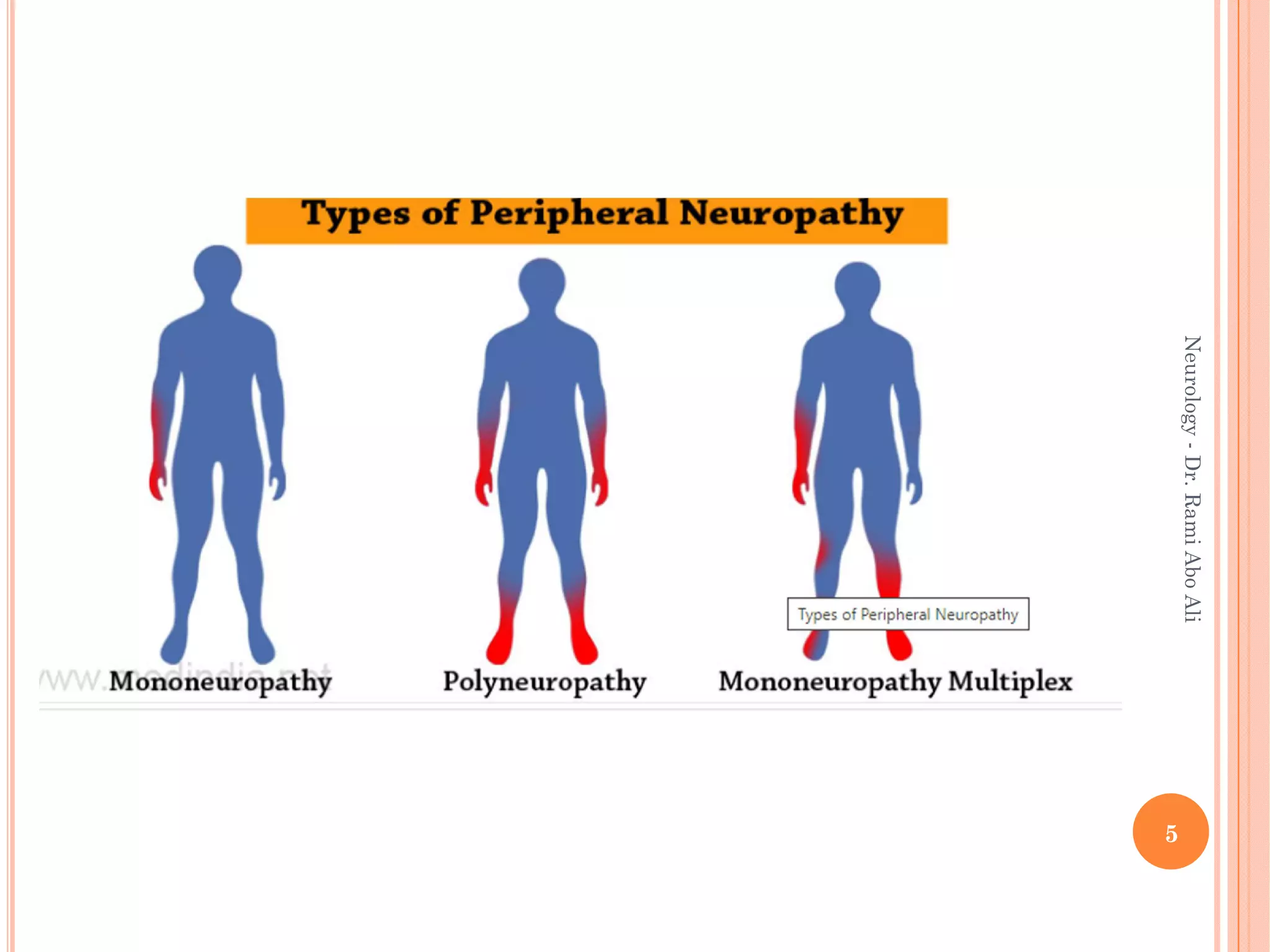
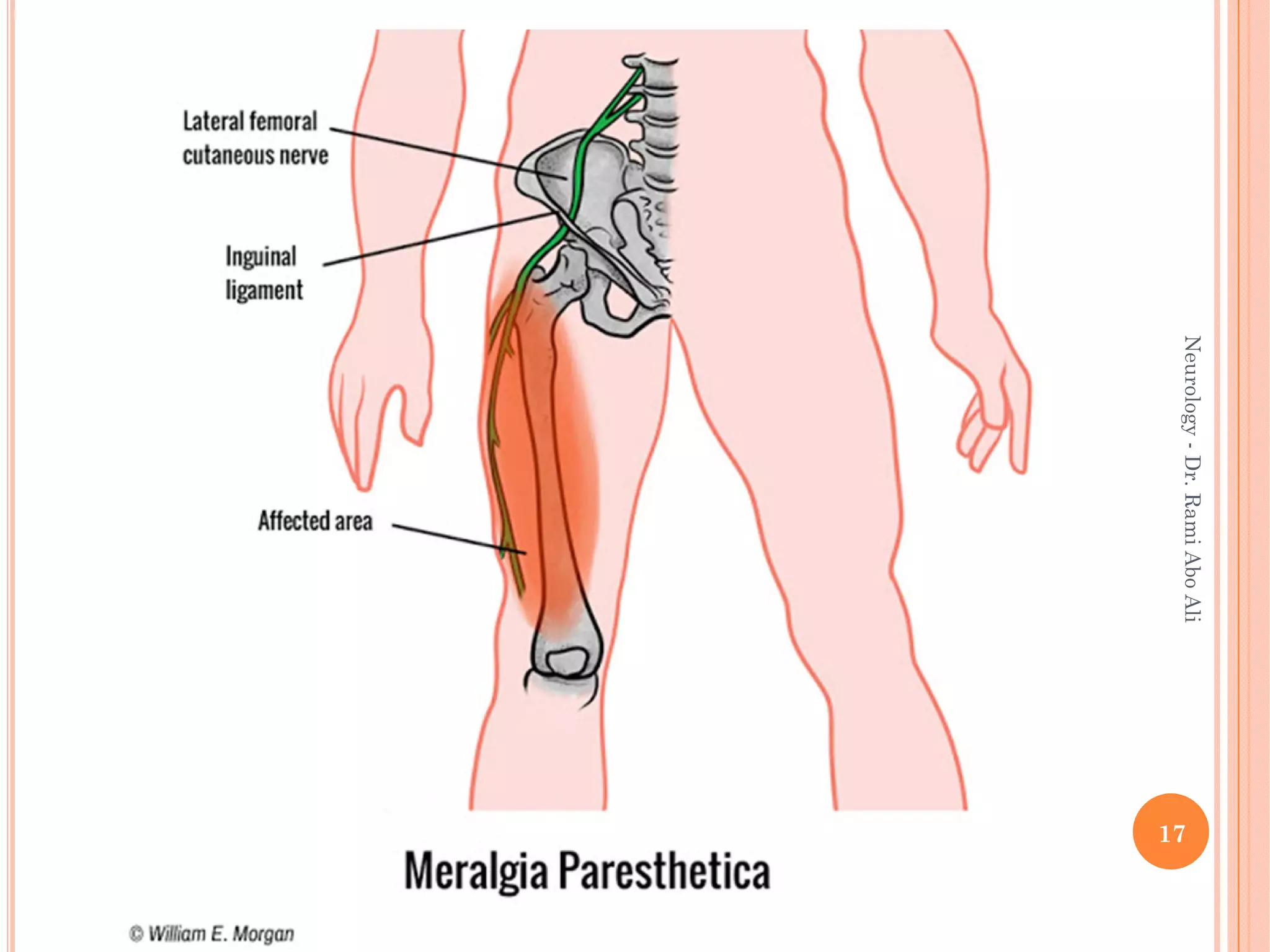
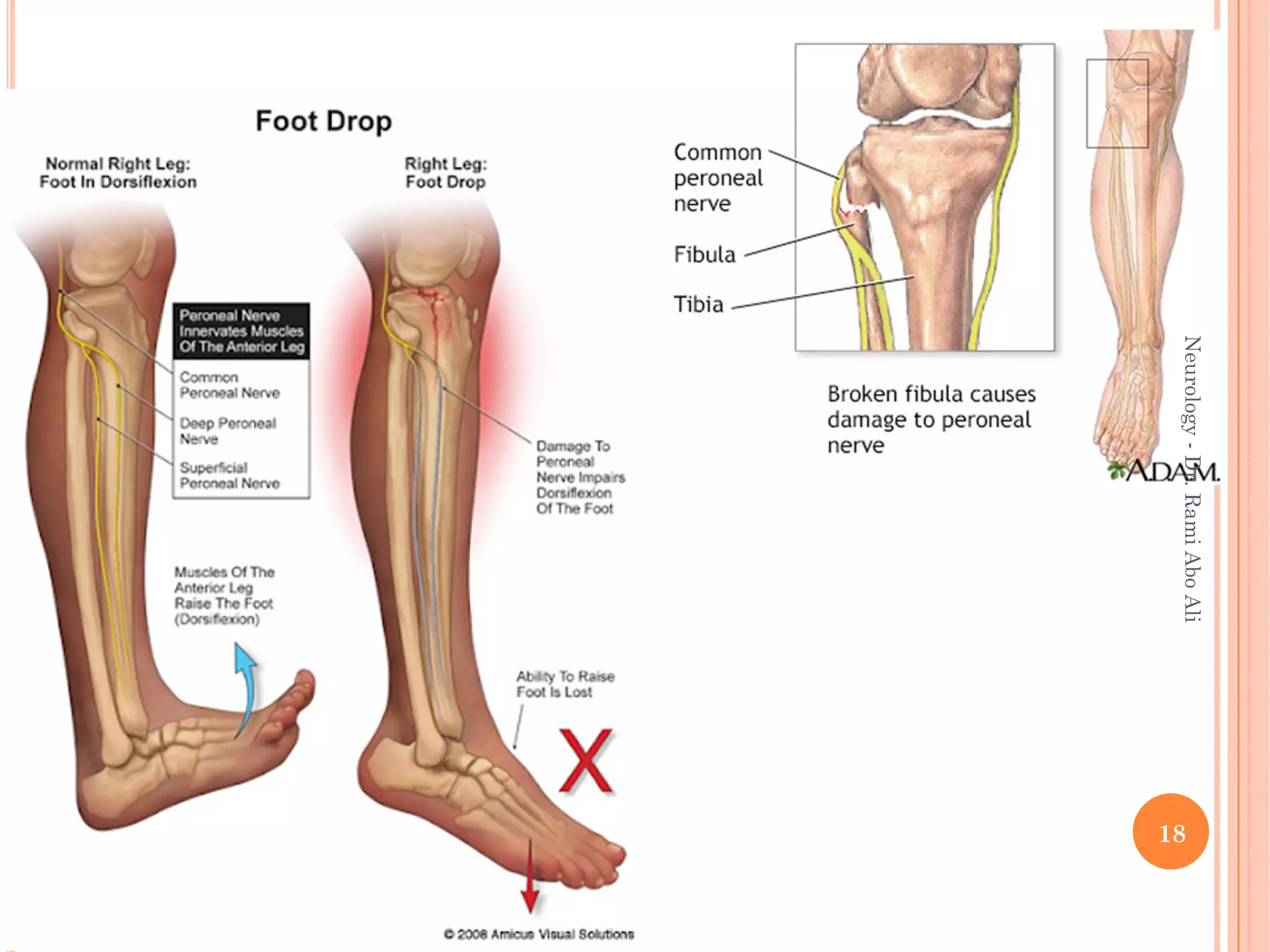
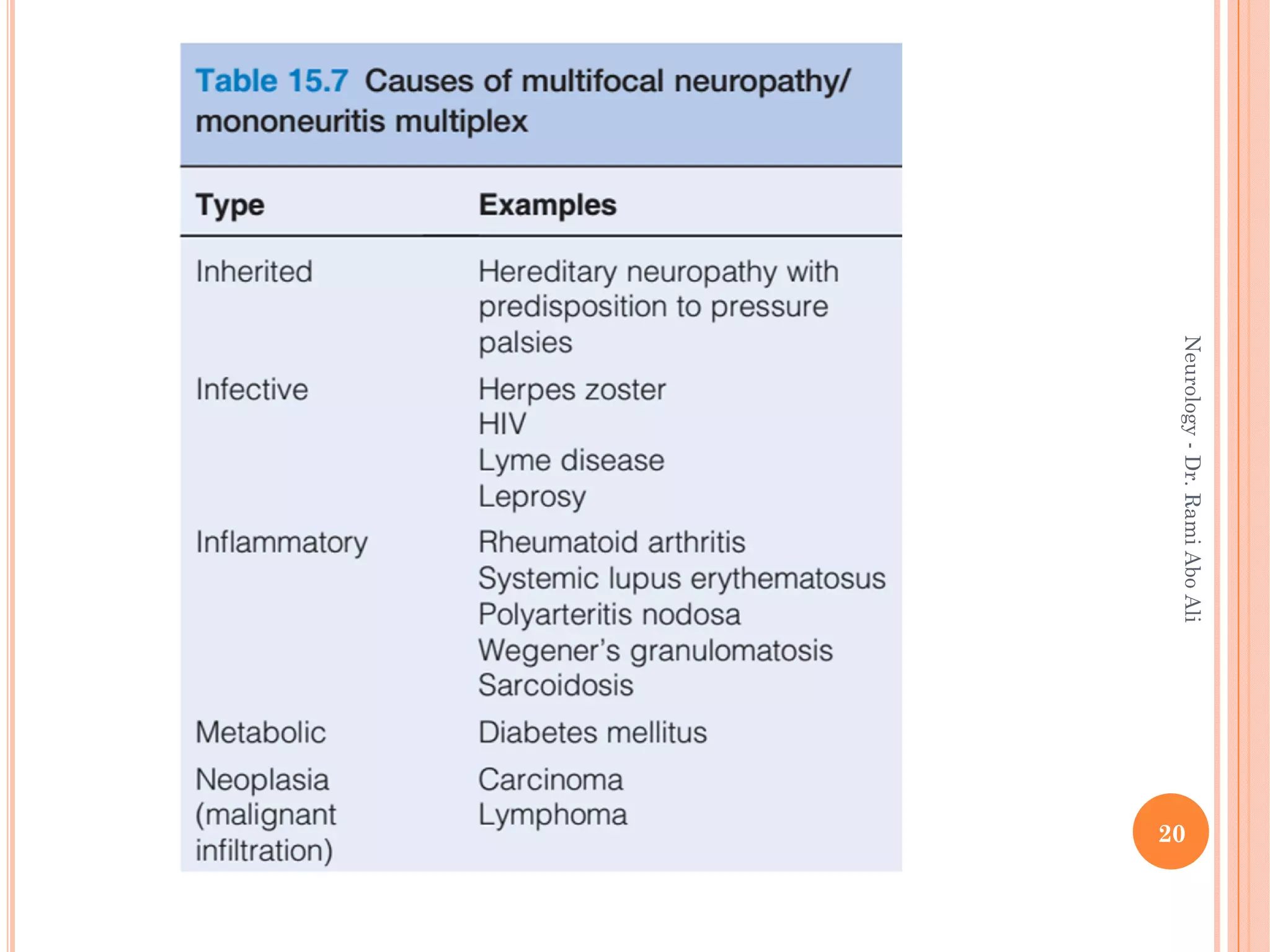
- Specific types discussed include mononeuropathies which affect individual nerves, polyneuropathies which affect multiple nerves symmetrically, and plexopathies.
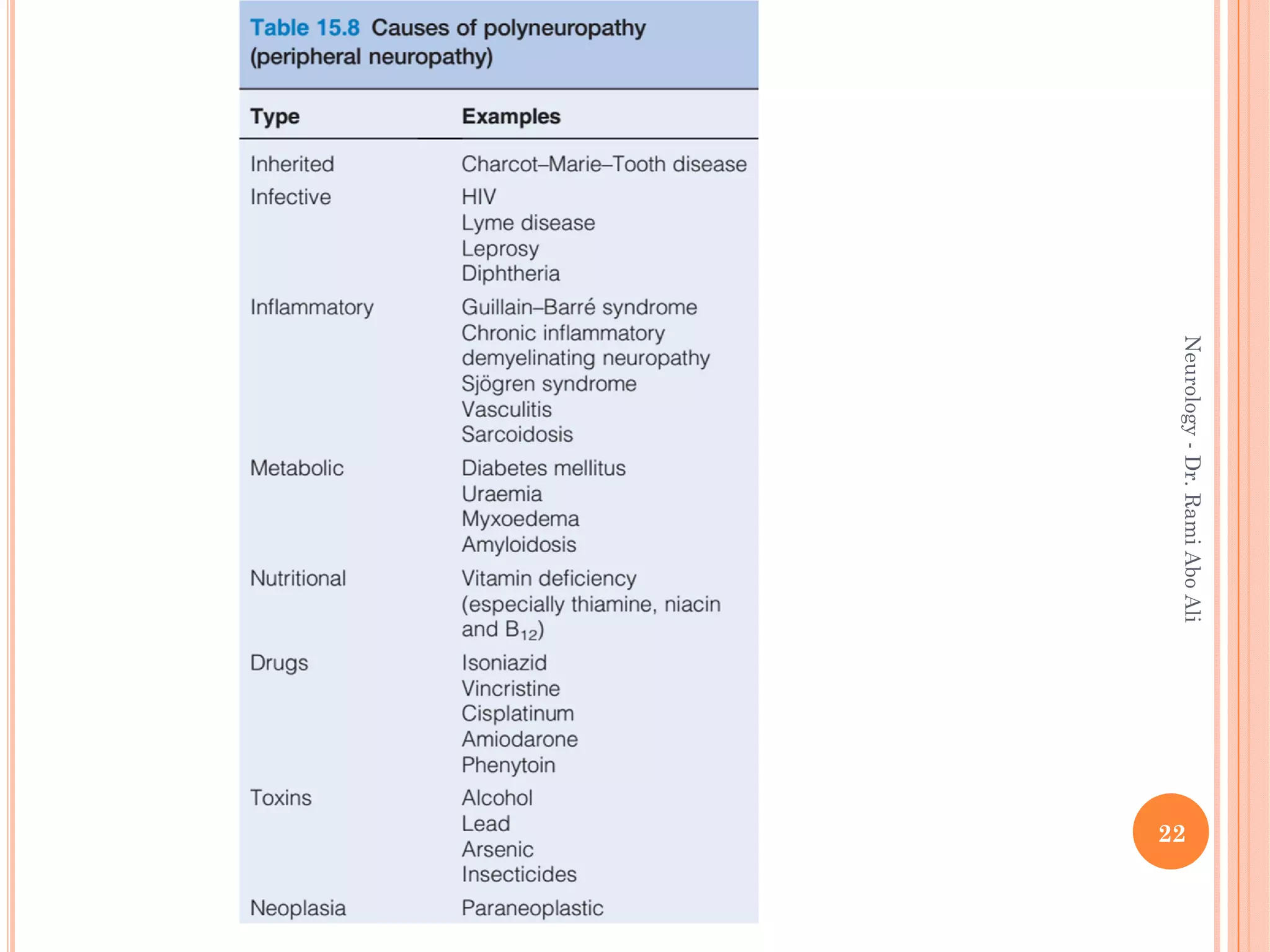
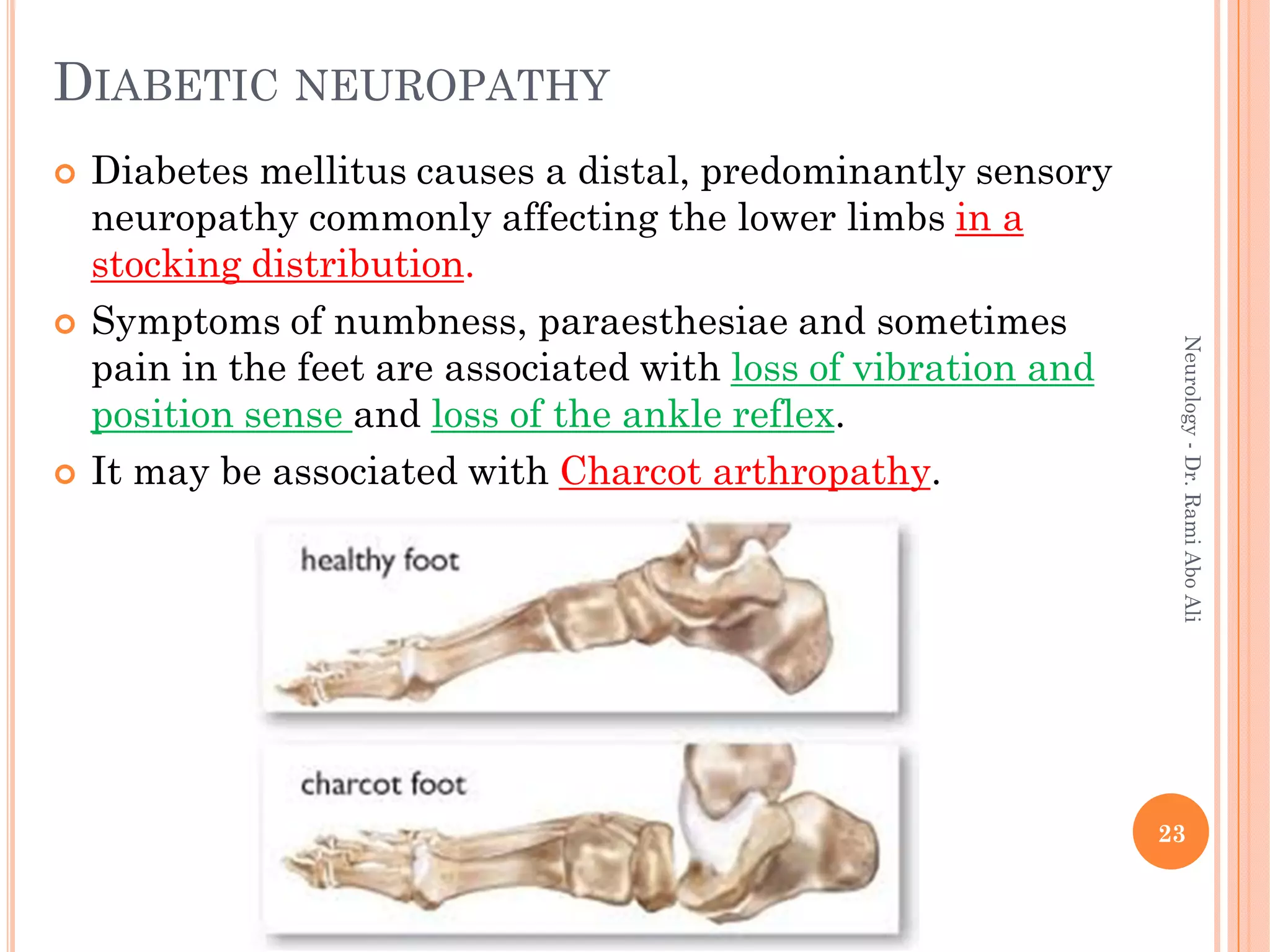
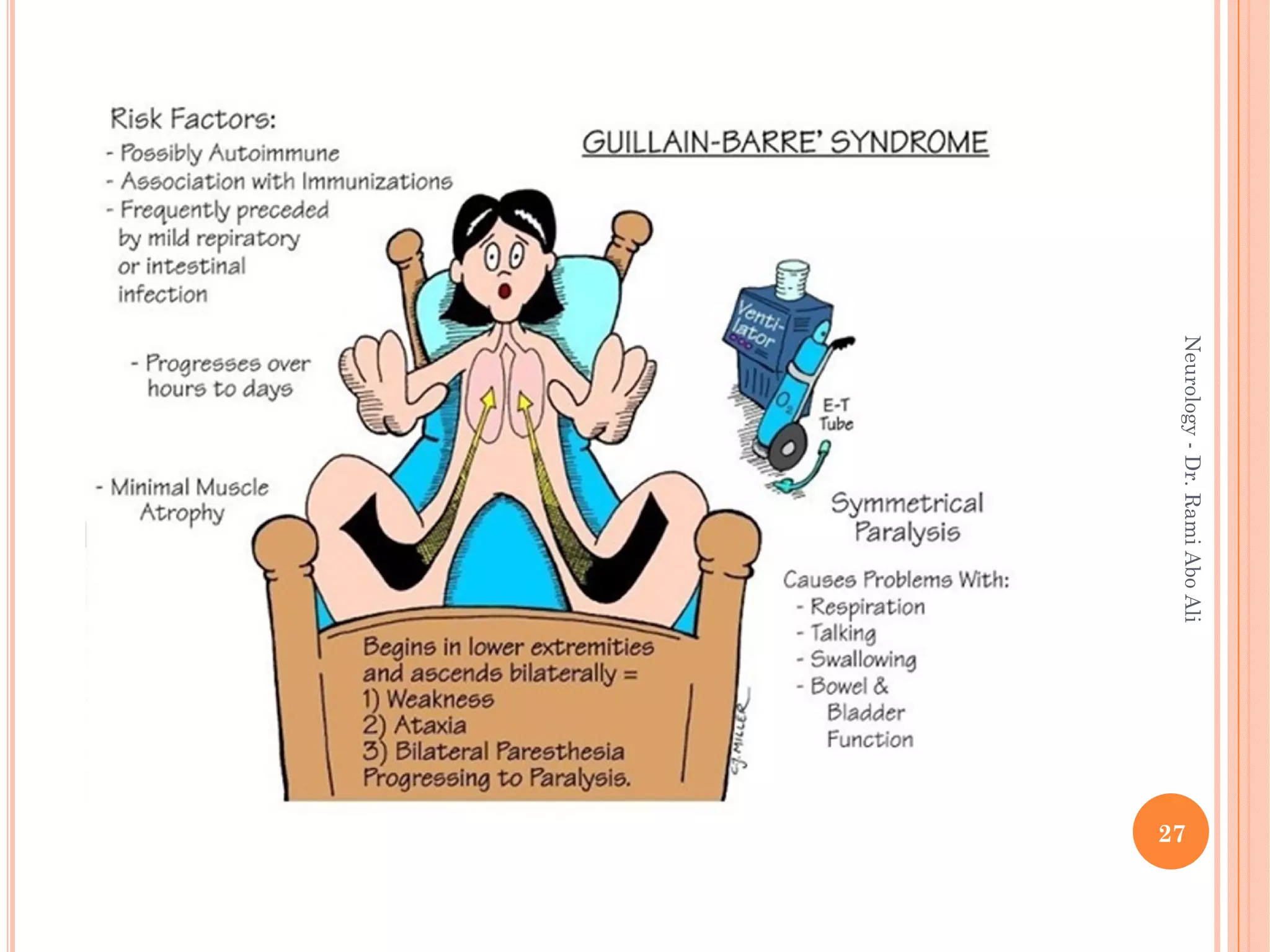
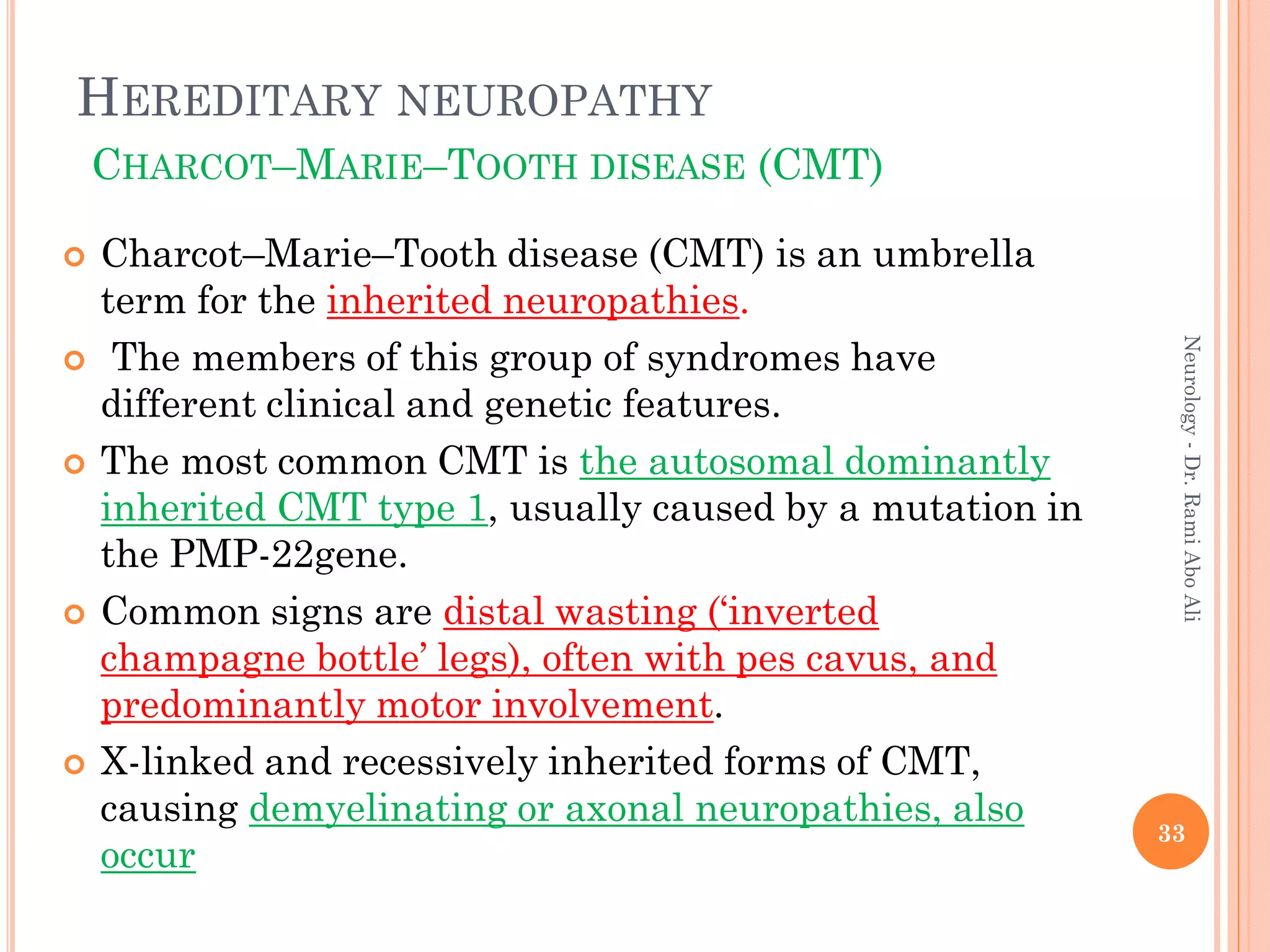
- Causes include metabolic, infectious, inflammatory, toxic, and hereditary factors. Specific conditions like diabetes, Guillain-Barré syndrome, and Charcot-Marie-Tooth disease are examined in depth.
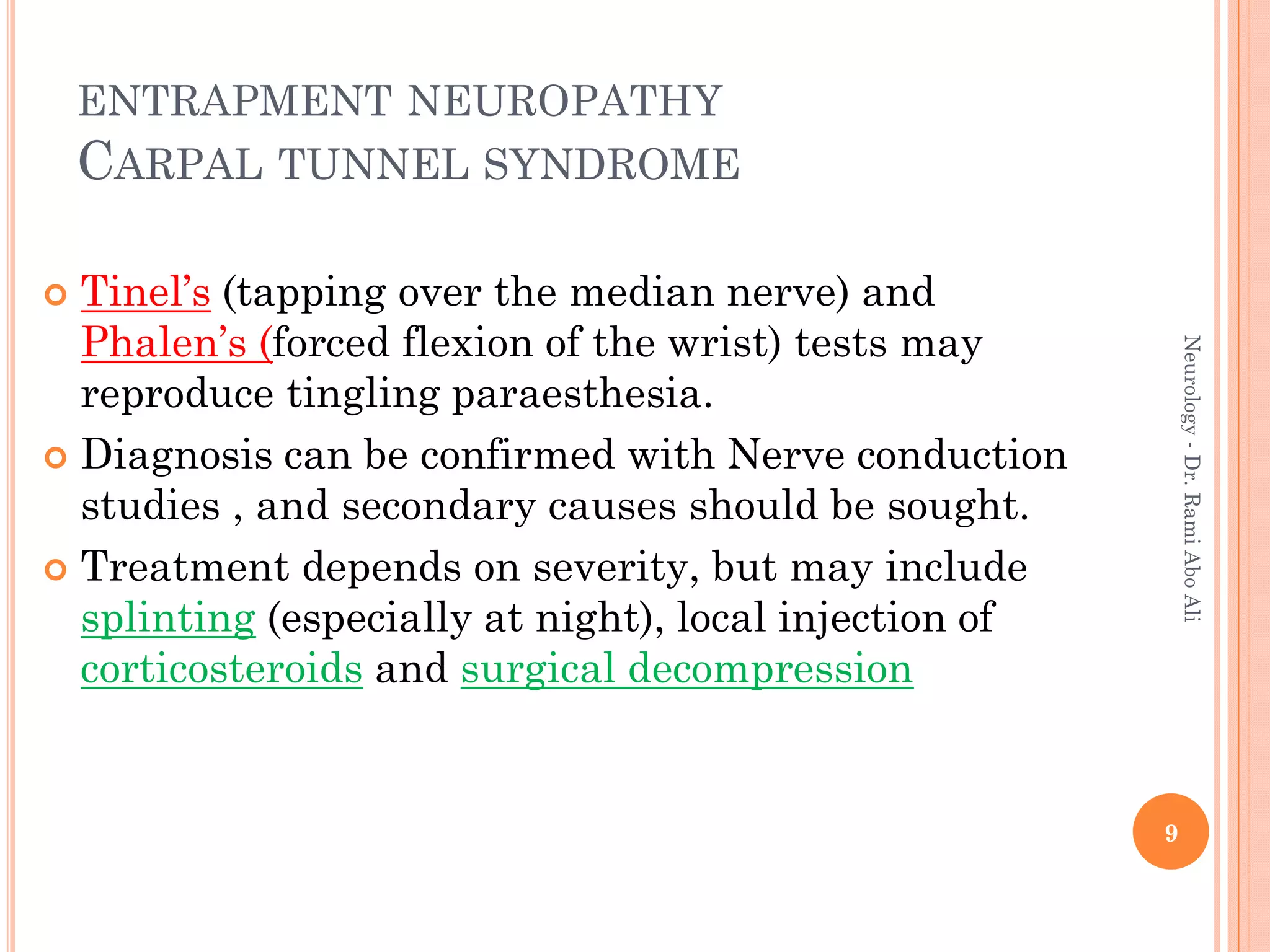
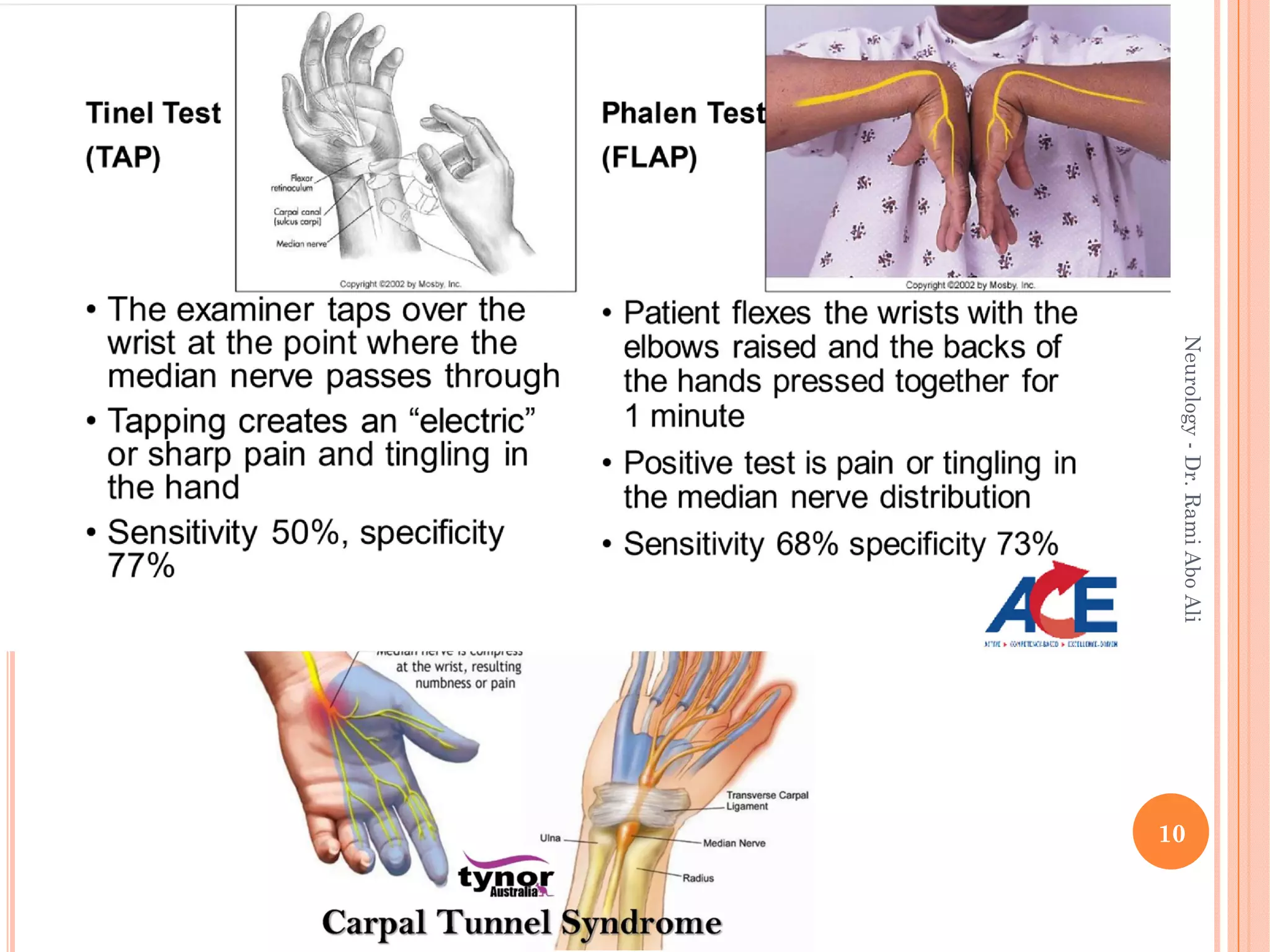
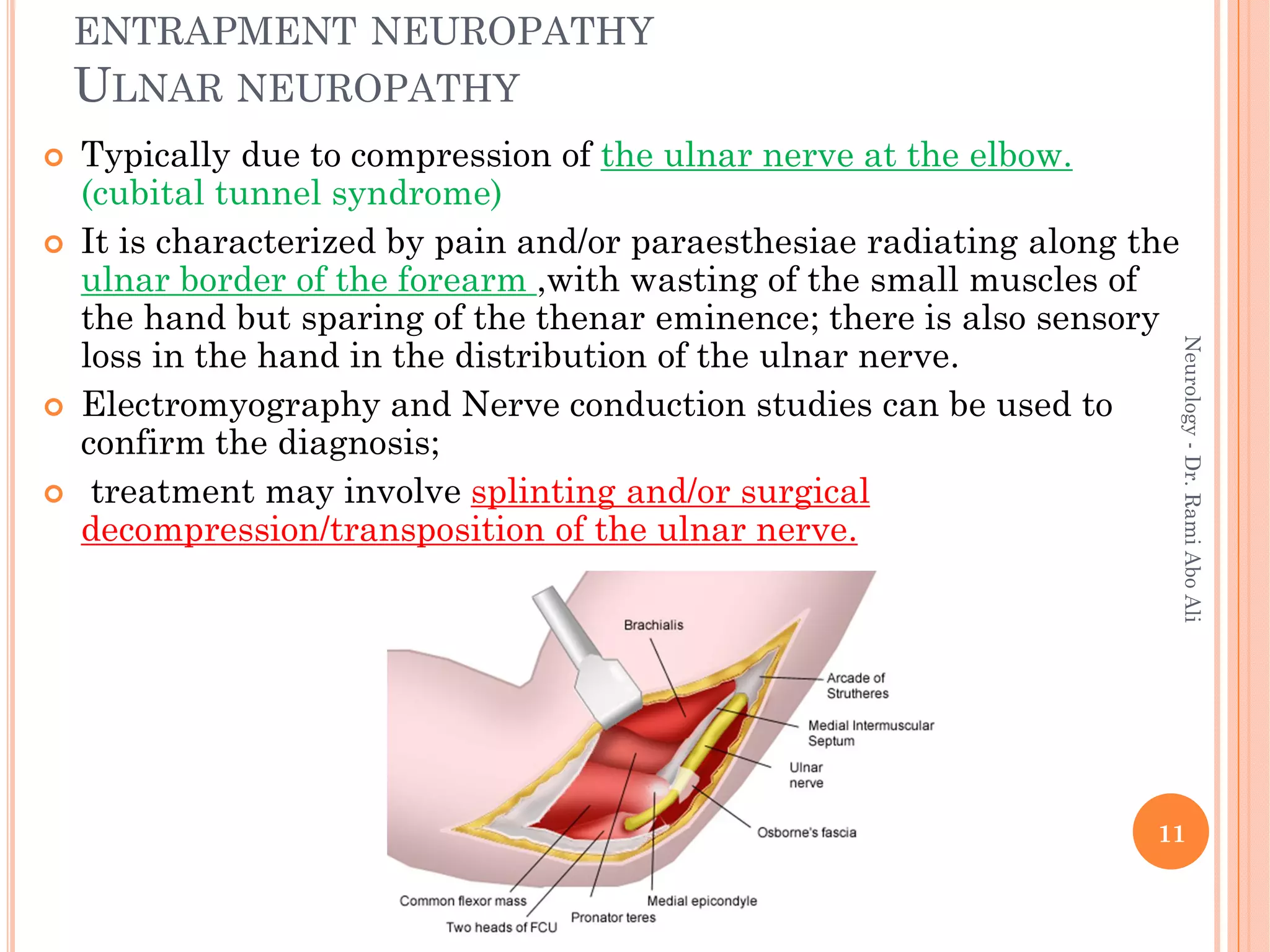
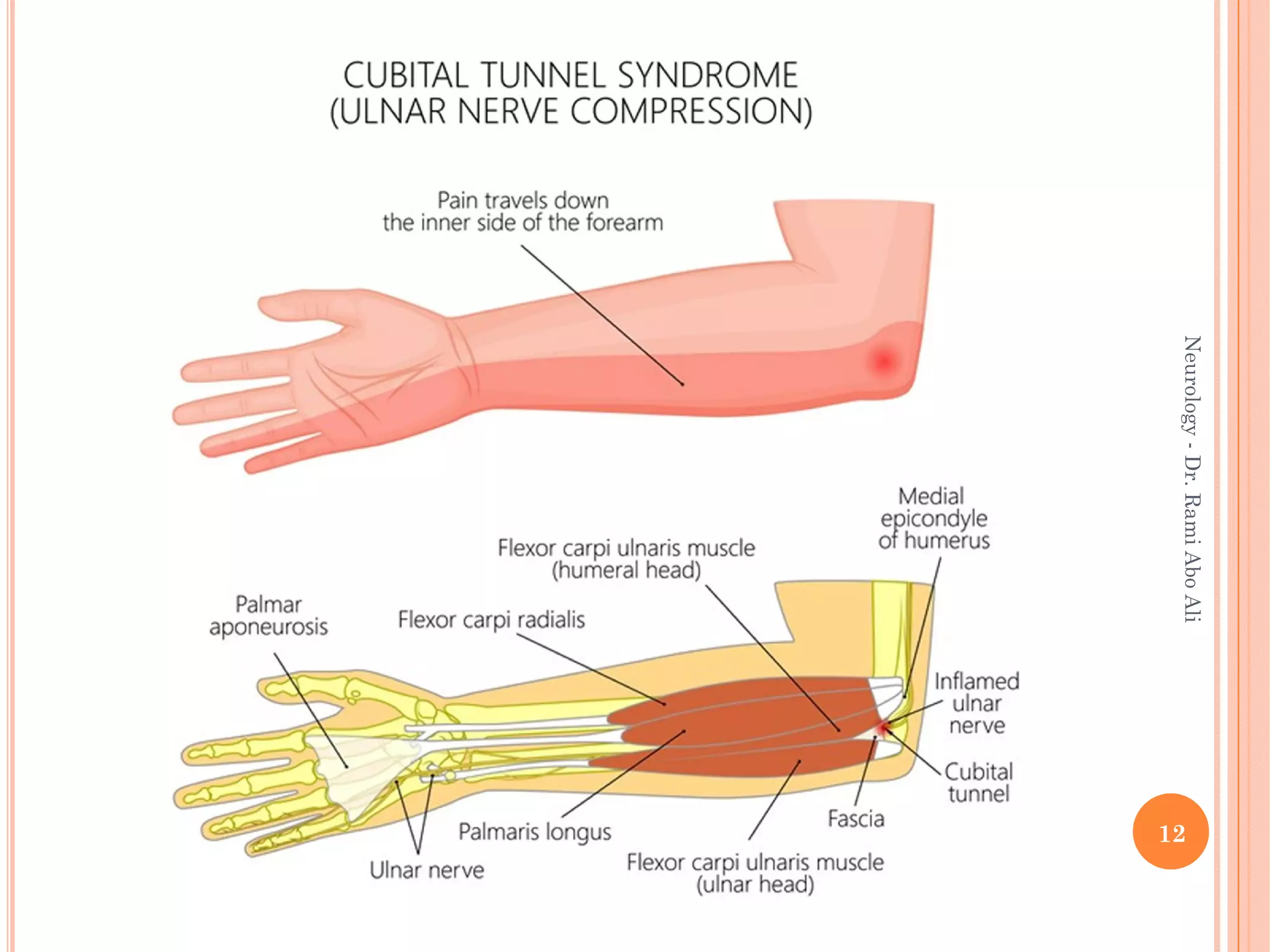
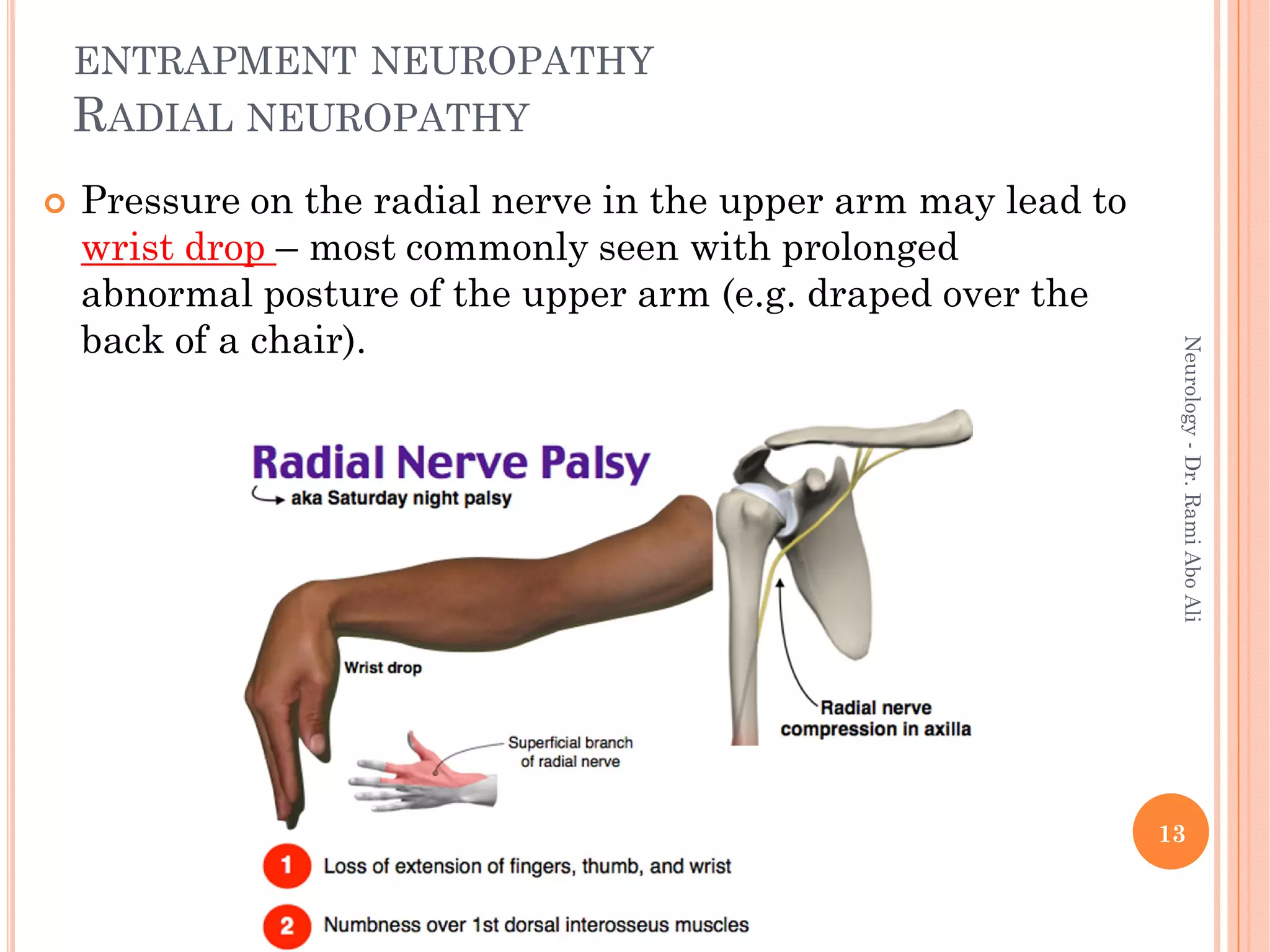
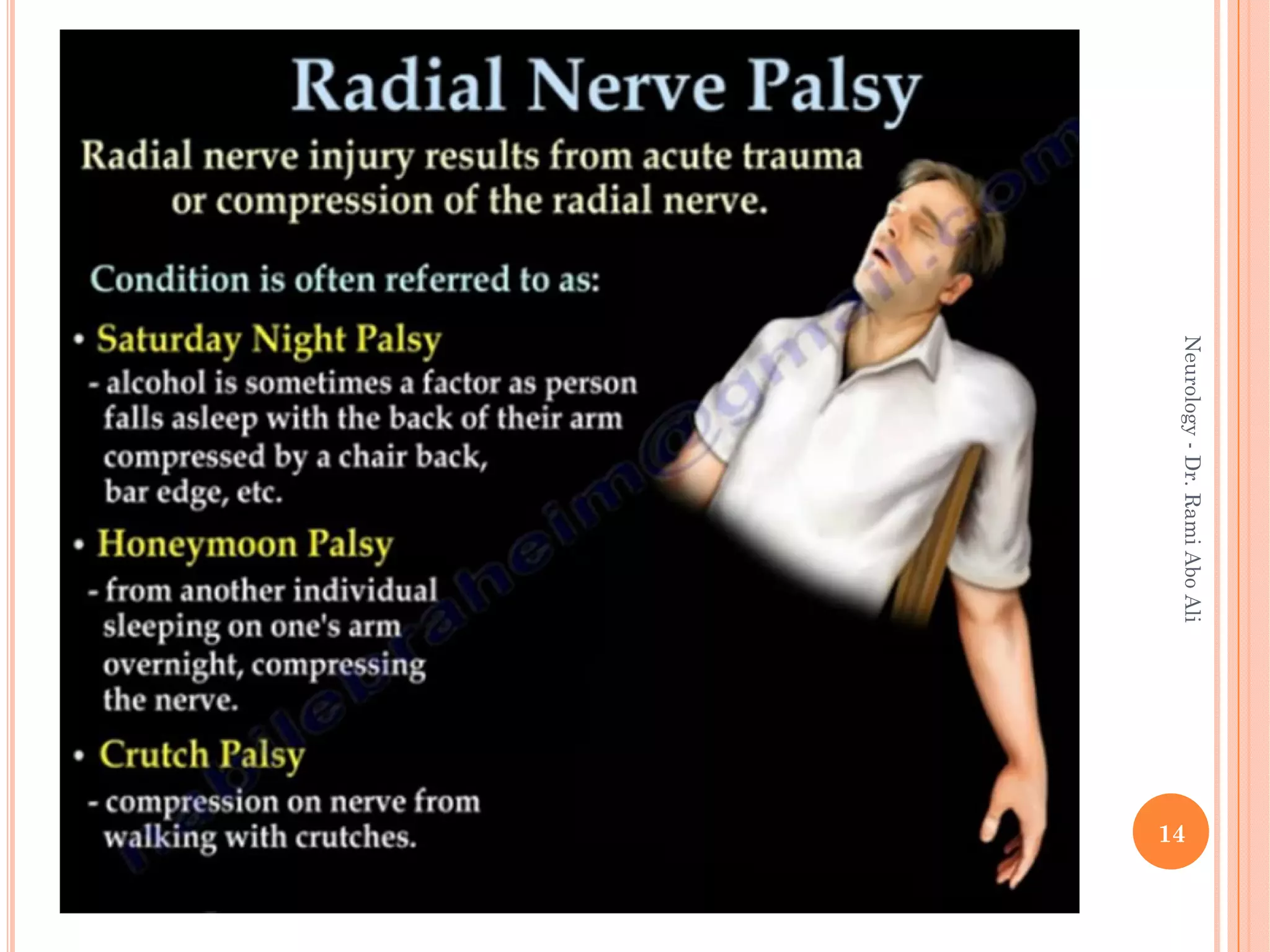
- Entrapment neuropathies at sites like the carpal

















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






