Downloaded 492 times



















































![Corresponding Author: Brian Sabb [email_address]](https://image.slidesharecdn.com/anteriorkneepainbydrbriansabb-129769317164-phpapp02/75/Anterior-Knee-Pain-By-Dr-Brian-Sabb-53-2048.jpg)

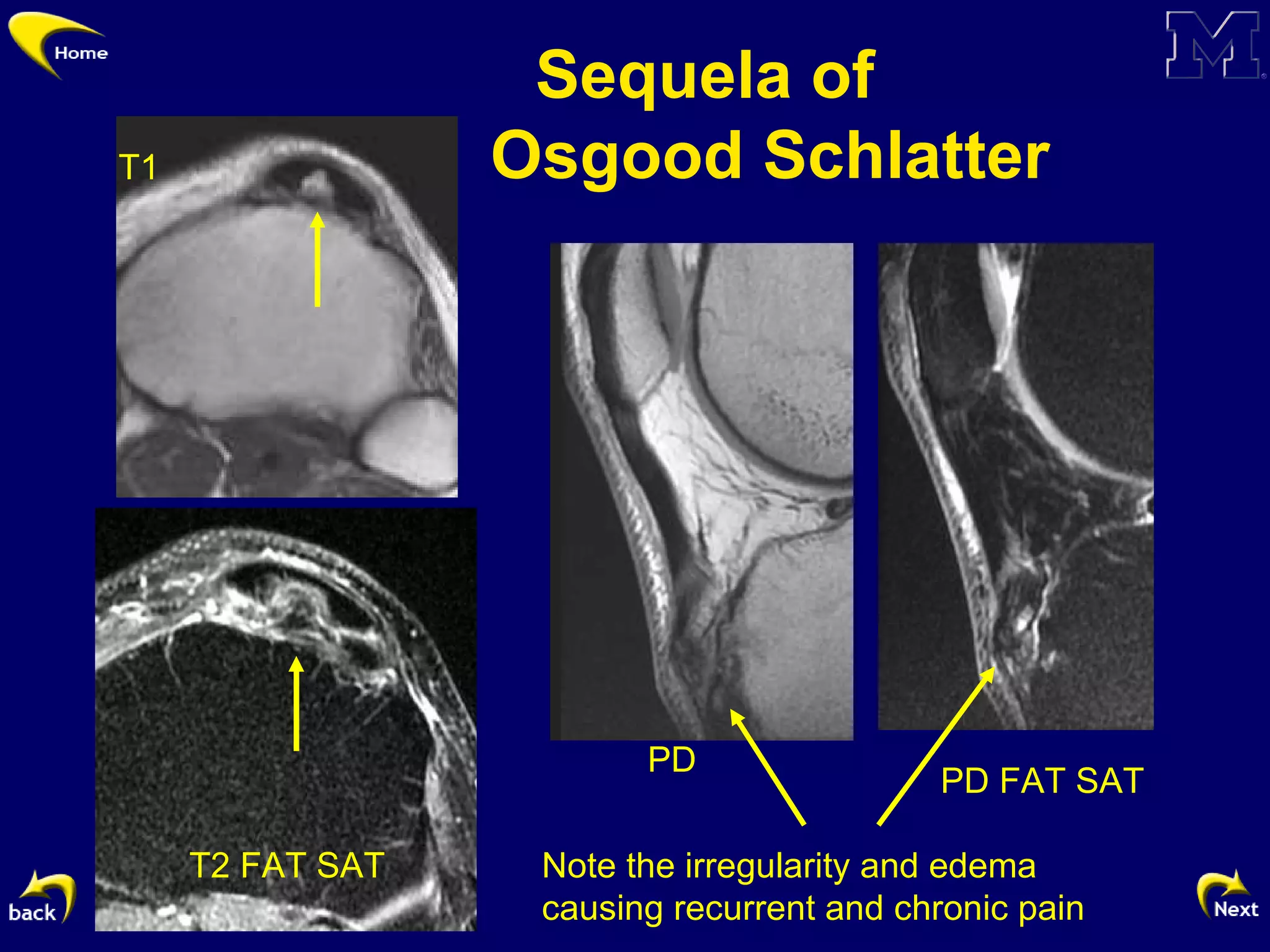
This document discusses the diagnostic challenges associated with anterior knee pain, focusing on various anatomical structures and conditions related to the patellofemoral joint. It highlights imaging findings from MRI and ultrasound for conditions such as prepatellar bursitis, infrapatellar fat pad pathology, and patellar tendon injuries. The article aims to enhance understanding of the biomechanics, pathophysiology, and relevant imaging techniques for diagnosing anterior knee pain.