Downloaded 1,237 times
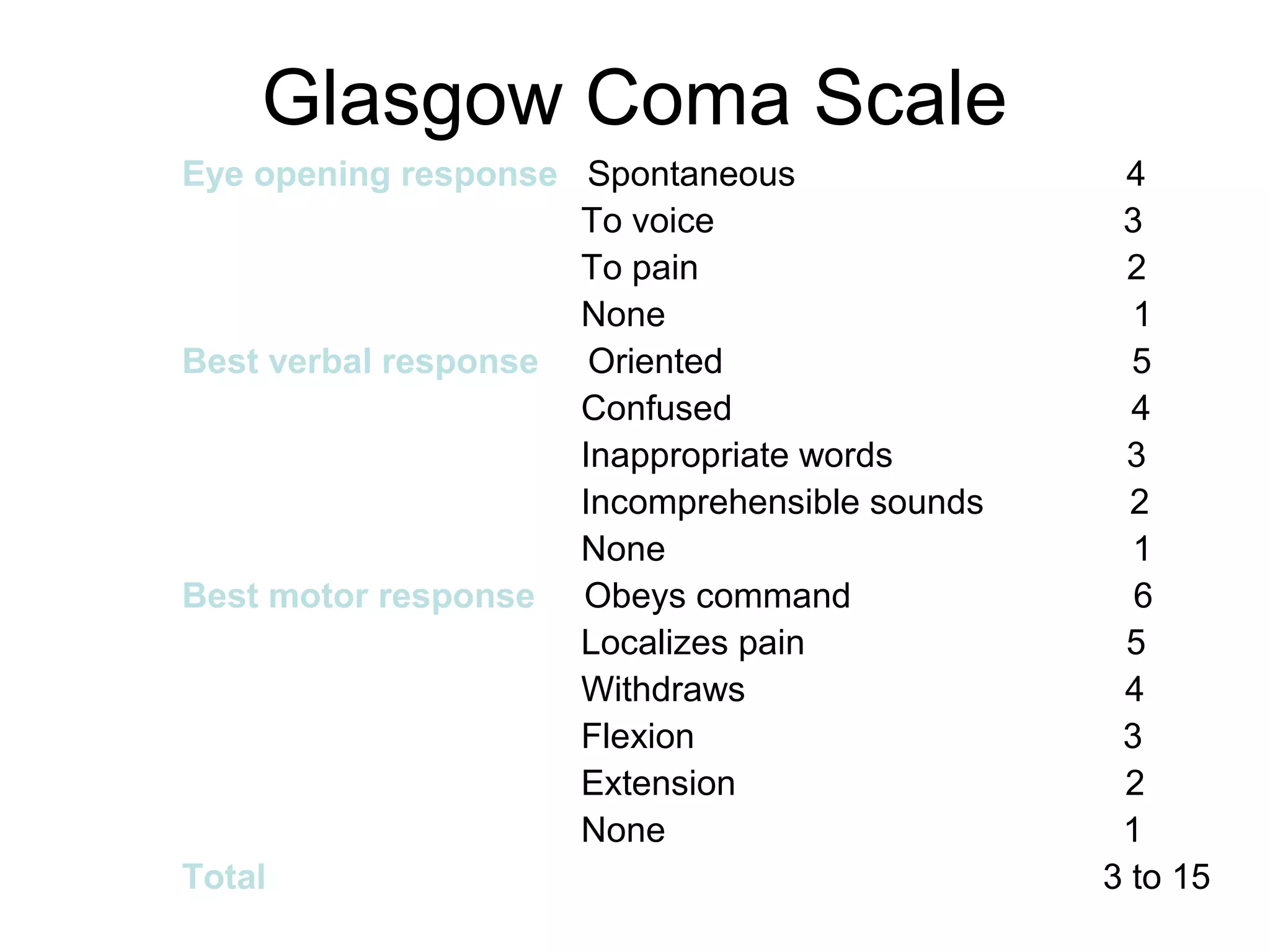

This document discusses the management of patients with neurologic dysfunction and altered levels of consciousness. It defines altered LOC as being less responsive to the environment. Causes can be structural, metabolic, or due to trauma, vascular disease, infection, tumors, metabolic derangements, hypoxia, or toxicity. Clinical manifestations range from subtle changes to coma. Nursing assessments include responsiveness, orientation, motor function and respiratory status. Interventions focus on airway protection, injury prevention, meeting fluid and nutrition needs, and skin and sensory integrity.























































































