Downloaded 47 times
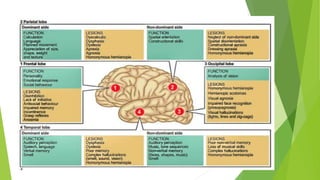






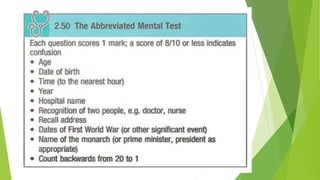
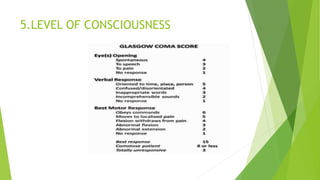





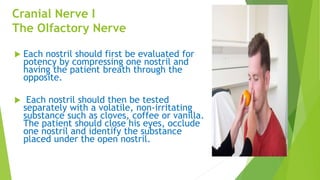






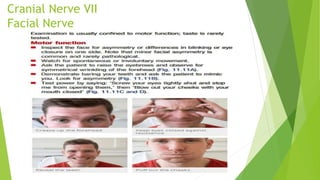
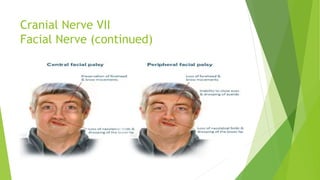


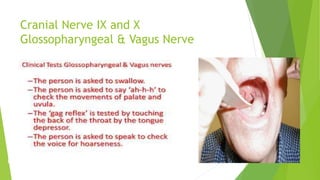
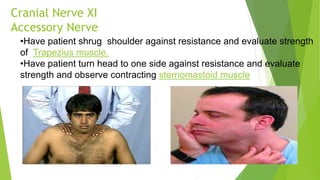
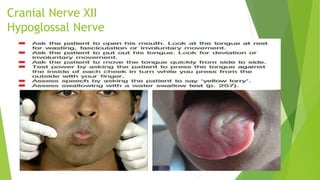


The document provides information about examining the nervous system. It discusses the components of the central and peripheral nervous systems. It then describes the equipment used in a nervous system examination and the various components assessed including higher mental functions, cranial nerve examination, motor and sensory system examination. It provides details on examining each of the 12 cranial nerves and describes various neurological conditions and abnormalities that may be observed.






















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















