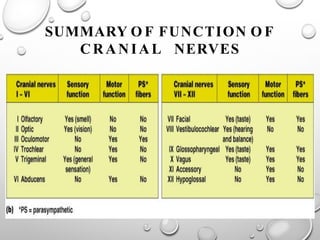
CRANIAL NERVES
I. Olfactory
II.Optic
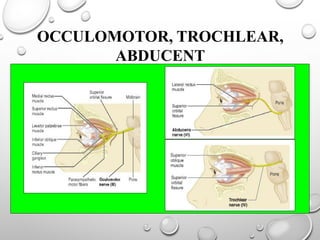
III. Occulomotor
IV. Trochlear
V. Trigeminal
VI. Abducent
VII. Facial
VIII. Auditory
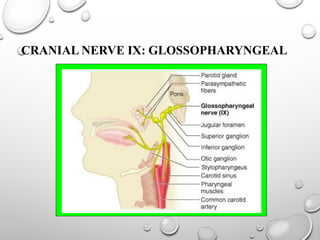
IX. Glossopharyngeal
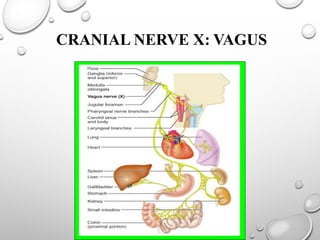
X. Vagus
XI. Spinal accessory
XII. Hypoglosseal
PURPOSE OF THETEST
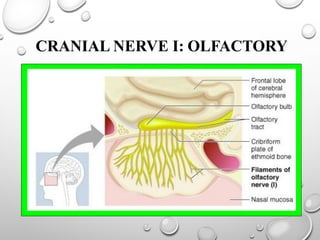
v To determine any impairment of smell is unilateral or
bilateral
v Whether impairment is due to any local nasal disease or
neural lesion.
8.
METHOD OF TESTING
vSmall bottles containing essences
of very familiar odour are
required
Ø Coffee
Ø Lemon
Ø Chocolate
Ø etc
9.
PROCEDURE
Compress 1 nostril& sniff the taste odour twice
Ask whether he can smell or identify odour
Repeat test on other nostril & ask if smell
is similar in both nostril
Allow odour to disperse & repeat test with other
2 test odour, ask he can distinguish smell
10.
INTERPRETATION OF RESULT
vWho can recognize & name odours quickly (females)
v Who can recognize but difficult in naming (males)
v Who can smell & know difference but neither recognize or naming.
ØThe above 3 should be accepted as normal
v Who feel each odour is similar but is distorted & unpleasant (parosmia).
v Those who can't smell anything or is much reduced compared to the other
(anosmia).
v Those whose responses are vague & variable
11.
COMMONCAUSES OFANOSMIA
Ø Acute/chronicinflammatory nasal disease
Ø Heavy smoking
Ø Head injury
Ø Intra cranial tumour compressing the olfactory bulb
Ø Atrophy of olfactory bulb
Ø Chronic meningeal inflammation
Ø Parkinson’s disease
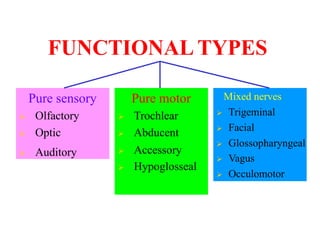
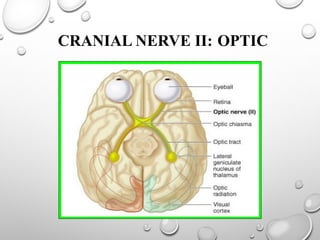
FUNCTION
v Carries thevisual impulses from the retina to the optic chiasma
& in the optic tract to the lateral geniculate body
v The impulse acts as an afferent pathway for the pupillary
light reflex.
14.
PURPOSE OF THETEST
v To measure aquity of vision & determine if any disease is due
to local occular disease or neural impairment.
v To chart the visual field.
15.
METHOD OF TESTING
vVisualacuity
ØThe standard snellen’s chart can
be used for vision & the Jaegar
type card can be used for near
vision.
[the commonest causes of visual
error lies in the eye only]
16.
VISUAL FIELD
v Purpose:
ØTo chart periphery of visual field
Ø To detect position, size & shape of the blind spot
17.
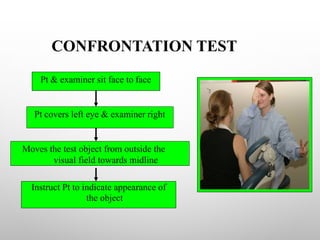
CONFRONTATION TEST
Instruct Ptto indicate appearance of
the object
Pt covers left eye & examiner right
Pt & examiner sit face to face
Moves the test object from outside the
visual field towards midline
18.
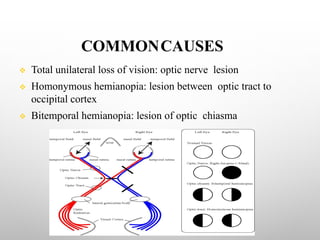
COMMONCAUSES
v Total unilateralloss of vision: optic nerve lesion
v Homonymous hemianopia: lesion between optic tract to
occipital cortex
v Bitemporal hemianopia: lesion of optic chiasma
FUNCTION
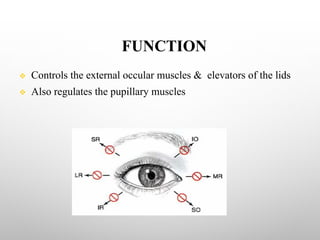
v Controls theexternal occular muscles & elevators of the lids
v Also regulates the pupillary muscles
21.
PURPOSE OF THETEST
Ø Inspect pupils to rule out a local disease, peripheral lesion
or a nuclear involvement.
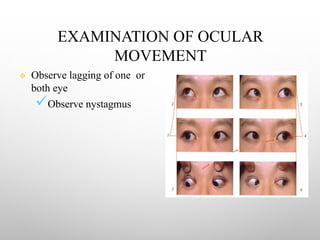
Ø Examine eye movement & determine if defects is
muscular origin or neural involvement.
Ø To detect nystagmus.
22.
METHOD OF TESTING
vObservation
ØPresence & absence of ptosis & squint
ØWhether unilateral or bilateral
ØConstant or variable
ØSize, shape, equality & regularity of the pupils
23.
REACTION TO LIGHT
ØReduce illumination of room & vision should focus on a
far object.
Ø A brightbeam of light is shone from the side of one eye.
Ø Repeat on the other side[the pupil should constrict briskly]
Ø Shield one eye & perform test on the other & see for
consensual reaction
24.
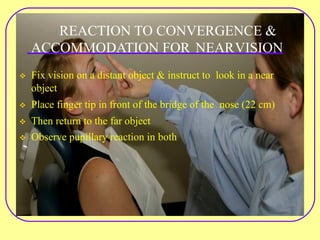
REACTION TO CONVERGENCE&
ACCOMMODATION FOR NEARVISION
v Fix vision on a distant object & instruct to look in a near
object
v Place finger tip in front of the bridge of the nose (22 cm)
v Then return to the far object
v Observe pupillary reaction in both
ANALYSIS OF DIPLOPIA
ØShield one eye with a transparent red shield
Ø Object is moved from left to right, up & down
Ø Ask if -
üHe sees 1 or 2 object
üObject lies one above the other or side by side
27.
RULES GOVERNING ANALYSISOF
DIPLOPIA
Ø Separation of image is greatest in the direction in which the
weak muscle has its purest action.
Ø False image is displaced farthest in the direction in which
the weak muscle should move the eye.
28.
ANALYZING NYSTAGMUS
Ø Watchthe patients eye while talking
Ø Ask to look at a definite point & move the point from left
to right & up to down
Ø Hold each end position for 5 sec & assess nystagmus
(direction, rate amplitude)
29.
COMMON CAUSES OFPARALYSIS
Ø Pontine lesions
Ø Neoplasms
Ø Vascular accidents
Ø Demyelinating disease
Ø Meningeal inflammation
Ø Tumor of base of skull
Ø Increased intra cranial pressure
Ø Head injury
[Total paralysis of III, IV & VI nerve indicates a lesion in
cavernous sinus (carotid aneurism)]
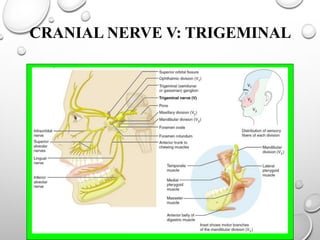
FUNCTION
v Carries allforms of sensation from the face, anterior scalp, eye
& the anterior 3rd of the tongue.
v Also supplies the muscles of mastication.
32.
PURPOSE OF THETEST
Ø To determine any sensory impairment.
Ø To determine unilateral or bilateral motor weakness &
determine UMN from LMN.
33.
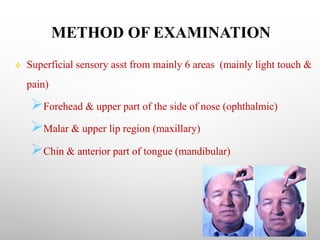
METHOD OF EXAMINATION
vSuperficial sensory asst from mainly 6 areas (mainly light touch &
pain)
ØForehead & upper part of the side of nose (ophthalmic)
ØMalar & upper lip region (maxillary)
ØChin & anterior part of tongue (mandibular)
34.
INTERPRETATION
Ø Total lossof sensation: lesion of ganglion or sensory root.
Ø Total sensory loss over 1 division: partial lesion of ganglion
or root.
Ø Touch only lost: pontine lesion affecting sensory nucleus.
Ø Pain & temp lost: dissociate anesthesia (seringobulbia).
35.
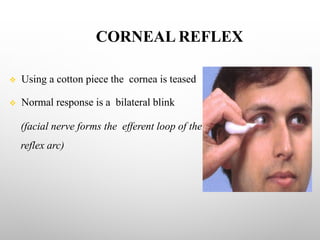
CORNEAL REFLEX
v Usinga cotton piece the cornea is teased
v Normal response is a bilateral blink
(facial nerve forms the efferent loop of the
reflex arc)
36.
INTERPRETATION
v No closure:ophthalmic division of the facial nerve.
v No response in either lid when abn. is tested & bilateral blink
when normal is tested: V nerve lesion
v No response of the affected side whichever side is tested:
VII nerve lesion.
37.
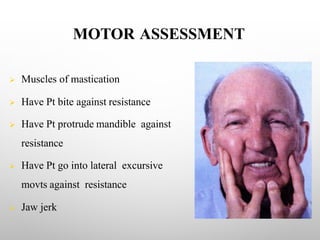
MOTOR ASSESSMENT
Ø Musclesof mastication
Ø Have Pt bite against resistance
Ø Have Pt protrude mandible against
resistance
Ø Have Pt go into lateral excursive
movts against resistance
Ø Jaw jerk
38.
COMMON CAUSES
v Tumorsof base of skull
v Chronic meningeal lesion
v Trigeminal sensory neuropathy
v Acoustic neuroma
v Syringomyelia
v Multiple sclerosis
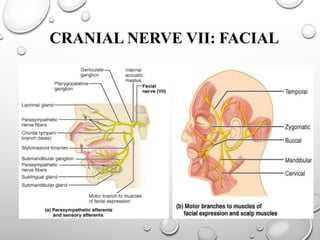
FUNCTION
v Supplies themuscles of facial expression including platysma
& stapedius muscle.
v Secretomotor fibers to the lacrimal gland & the salivary gland.
v Carries sensation of taste from anterior 2/3 of tongue & general
sensation from external acoustic meatus.
41.
PURPOSE OF THETEST
v To detect any unilateral or bilateral weakness of facial muscles
(UMN or LMN)
v Detect impairment of taste
42.
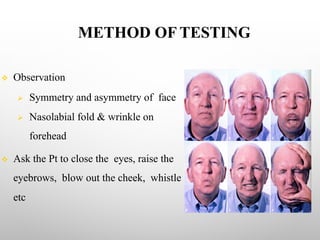
METHOD OF TESTING
vObservation
Ø Symmetry and asymmetry of face
Ø Nasolabial fold & wrinkle on
forehead
v Ask the Pt to close the eyes, raise the
eyebrows, blow out the cheek, whistle
etc
43.
EXAMINATION OF TASTE
vThe four primary taste (sweet, salt, sour, bitter) can be
carried out by using sugar, salt, vinegar & quinine
v The side of the tongue is moistened by the test substance
v Ask the Pt to indicate taste by pointing
44.
SECRETOMOTOR FUNCTION
Ø Theflow of tears of two side can be compared by giving
ammonia to inhale which will result in tearing of eye.
Ø The flow of saliva can be tasted by keeping a spicy substance in
the tongue & the tip is raised to observe the sub maxillary
salivary flow.
45.
REFLEXES
Ø Corneal reflex
ØNasopalpebral reflex: tap on the nasopalpebral ridge will
produce closure of both eyes. In bells palsy there is failure to
close on the affected side
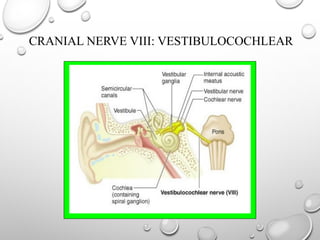
FUNCTION
v Carries theimpulses of sound from the hair cell of organ of
corti to cochlear nucleus in pons
v Control balance through vestibular nerve
49.
PURPOSE OF THETEST
v To determine any deafness is bilateral or unilateral
v Whether deafness is due disease of middle ear or cochlear nerve
v To determine the disturbance of vestibular functions
50.
TEST OF HEARING
vObserve if the patient turns one ear
towards you
v Evaluate hearing using a ticking
watch, rub fingers together, whisper.
51.
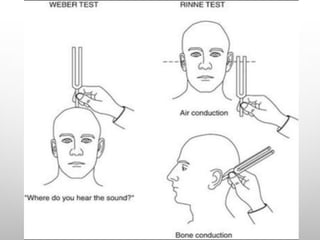
RINNE’STEST
Ø Strike atuning fork gently, hold it near one external meatus
& ask the pt if he can hear it.
Ø Place it on the mastoid, ask if he can still hear it & instruct
him to say “NOW” when sound ceases, & keep it on the
external meatus again (normally the note is still audible).
53.
INTERPRETATION
v In middleear deafness – the note is not heard
v In nerve deafness – air & bone conduction are reduced.
54.
WEBER’S TEST
v Thefork is place on the vertex
v Ask the Pt if he can hear the sound all over the head, in both
ears or in one ear
v In nerve deafness the sound appear to be heard on the
normal ear
v On chronic middle ear disease it is conducted to the abnormal ear
55.
COMMONCAUSES OF DEAFNESS
ØDisease of external & middle ear & Eustachian tube
Ø Prolonged exposure to loud noise
Ø Old age
Ø Meningitis
Ø Demyelinating disease
Ø Deafness due to drugs
56.
TEST OF VESTIBULARFUNCTION
Ø Observe equilibrium as patient walks or
stands
Ø Observe abnormal eye movts
Ø Ask for -
• Dizziness
• Falling
• Nausea and vomiting
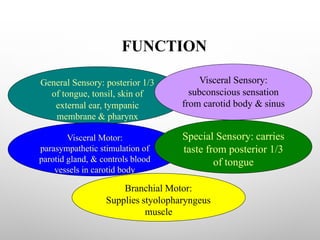
FUNCTION
General Sensory: posterior1/3
of tongue, tonsil, skin of
external ear, tympanic
membrane & pharynx
Visceral Motor:
parasympathetic stimulation of
parotid gland, & controls blood
vessels in carotid body
Visceral Sensory:
subconscious sensation
from carotid body & sinus
Special Sensory: carries
taste from posterior 1/3
of tongue
Branchial Motor:
Supplies styolopharyngeus
muscle
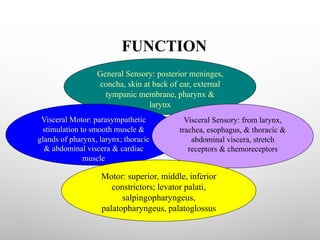
FUNCTION
General Sensory: posteriormeninges,
concha, skin at back of ear, external
tympanic membrane, pharynx &
larynx
Visceral Motor: parasympathetic
stimulation to smooth muscle &
glands of pharynx, larynx; thoracic
& abdominal viscera & cardiac
muscle
Visceral Sensory: from larynx,
trachea, esophagus, & thoracic &
abdominal viscera, stretch
receptors & chemoreceptors
Motor: superior, middle, inferior
constrictors; levator palati,
salpingopharyngeus,
palatopharyngeus, palatoglossus
61.
PURPOSE OF THETEST
v To test the elevation of palate & contraction of pharynx
v To examine the movts of vocal cords
[note: the IX & X nerve are tested together]
62.
METHOD OF TESTING
vNotice the pitch & quality of voice, cough & difficulty in
swallowing saliva
v Ask the Pt to open his mouth wide after a few movts ask to
say “AH” while breathing out & “UGH” while in
v The palate should move symmetrically upwards & backwards,
the uvula in midline & two sides of pharynx contract
symmetrically
63.
COMMONCAUSES OF LESION
vPoliomyelitis
v Syringobulbia
v Posterior fossa tumor
v Advanced parkinsonism
v Myasthenia gravis
v Enlarged cervical glands
v Surgical operation of the neck
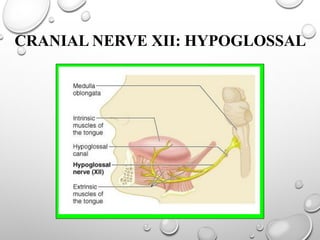
FUNCTION
v Control movtsof the tongue, hyoid bone& larynx during
& after deglutition
Supplies 3 of 4 extrinsic
muscles of tongue & all
intrinsic muscles of
tongue
71.
PURPOSE OF THETEST
v To inspect the surface of the tongue
v To detect wasting, weakness & involuntary movts
v To examine voluntary muscle control
72.
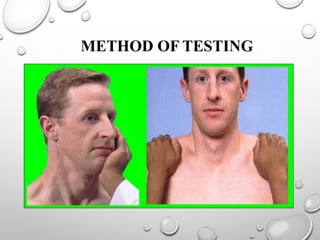
METHOD OF TESTING
vAsk the Pt to protrude the tongue &
observe for
ØReduction in size of affected side
ØExcessive ridging & wrinkling
ØRestricted protrusion
ØDeviation towards one side


![METHOD OF TESTING
v Visualacuity
ØThe standard snellen’s chart can
be used for vision & the Jaegar
type card can be used for near
vision.
[the commonest causes of visual
error lies in the eye only]](https://image.slidesharecdn.com/cranialnerveexamination-250427091512-0f77e785/85/Cranial-Nerve-Examination-15-320.jpg)
![REACTION TO LIGHT
Ø Reduce illumination of room & vision should focus on a
far object.
Ø A brightbeam of light is shone from the side of one eye.
Ø Repeat on the other side[the pupil should constrict briskly]
Ø Shield one eye & perform test on the other & see for
consensual reaction](https://image.slidesharecdn.com/cranialnerveexamination-250427091512-0f77e785/85/Cranial-Nerve-Examination-23-320.jpg)
![COMMON CAUSES OF PARALYSIS
Ø Pontine lesions
Ø Neoplasms
Ø Vascular accidents
Ø Demyelinating disease
Ø Meningeal inflammation
Ø Tumor of base of skull
Ø Increased intra cranial pressure
Ø Head injury
[Total paralysis of III, IV & VI nerve indicates a lesion in
cavernous sinus (carotid aneurism)]](https://image.slidesharecdn.com/cranialnerveexamination-250427091512-0f77e785/85/Cranial-Nerve-Examination-29-320.jpg)
![PURPOSE OF THE TEST
v To test the elevation of palate & contraction of pharynx
v To examine the movts of vocal cords
[note: the IX & X nerve are tested together]](https://image.slidesharecdn.com/cranialnerveexamination-250427091512-0f77e785/85/Cranial-Nerve-Examination-61-320.jpg)