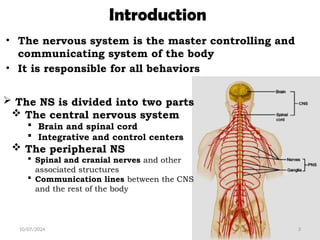
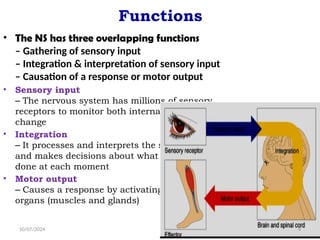
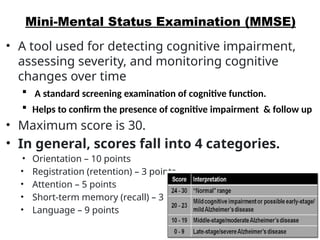
The document provides an overview of the nervous system, detailing its components, functions, and the clinical examination associated with it. It outlines the structure of the central and peripheral nervous systems, describes neurological evaluation techniques, and lists various tests and assessments such as the Glasgow Coma Scale and the Mini-Mental Status Examination. Key elements include the assessment of mental status, cranial nerves, and motor/sensory functions, along with the interpretation of findings from neurological examinations.


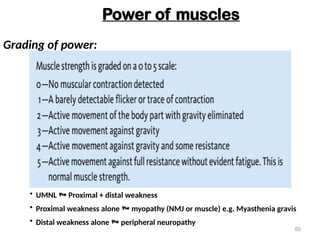
![Glasgow Coma Scale (GCS)
10/07/2024 14
• A method used to assess the level of consciousness more objective
GCS Score:= (E[4] + V[5] + M[6])
= Best possible score 15;
= Worst possible score 3.](https://image.slidesharecdn.com/8-241007054419-7ec0810e/85/8-Nervous-system-pptxEEEEEEEEEEEEEEEEEEEEEEEEE-14-320.jpg)
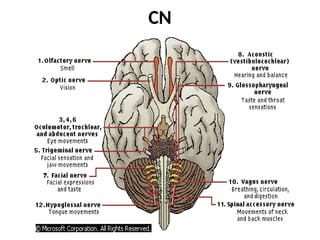
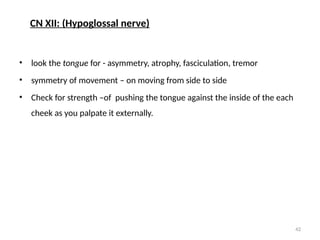
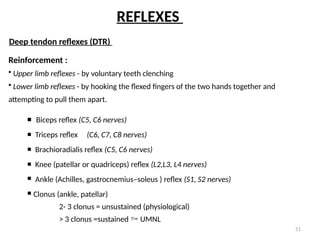
![C.
Nerve
Other Name Functions Superficial Exit Level
CN I Olfactory n. Smell
Olfactory bulb [superior to B. Stem]
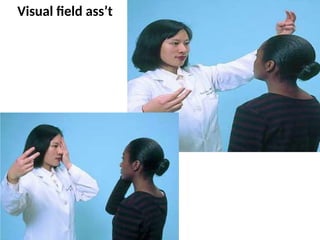
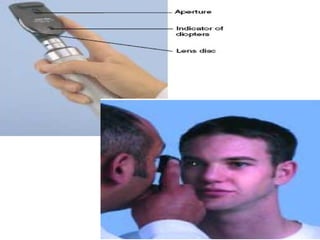
CN II Optic Visual acuity, visual fields, and ocular fundi Optic chiasm [superior to B. Stem]
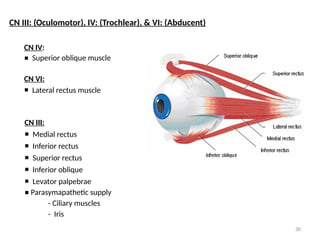
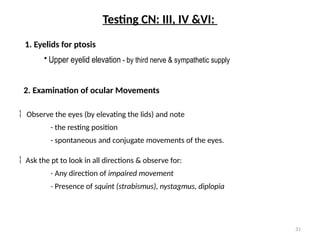
CN III Oculomotor EOM movements Medial midbrain
CN IV Trochlear EOM movements Dorsal midbrain
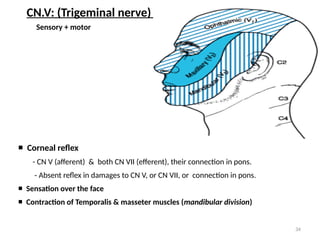
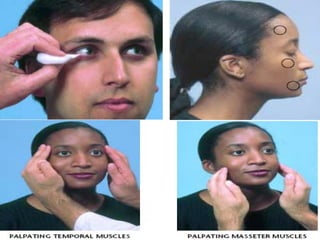
CN V Trigeminal Corneal reflexes, facial sensation, and jaw movements
Sen Corneal reflex, Sensation over the face
Mot muscle of Mastication
Pons
CN VI Abducent EOM movements Pons
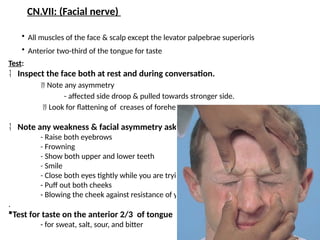
CN VII Facial Facial movements
Mot muscles of the face & scalp
Sen Ant 2/3 of the tongue taste
Pons
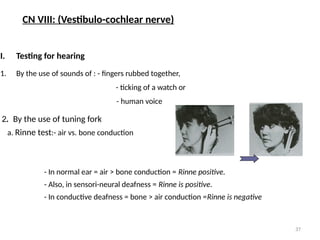
CN VIII Vestibulocochlear Hearing and balance Rostral medulla
CN IX Glossopharyngeal Swallowing and rise of the palate, gag reflex
The taste of posterior third of tongue
Rostral medulla
CN X Vagus Rostral medulla
CN XI Spinal Accessory Shoulder and neck movements Spinal C1-C6
CN XII Hypoglossal Tongue symmetry, position, and movement Rostral Medulla
CRANIAL NERVES (CN)](https://image.slidesharecdn.com/8-241007054419-7ec0810e/85/8-Nervous-system-pptxEEEEEEEEEEEEEEEEEEEEEEEEE-23-320.jpg)