
Recommended
More Related Content
Similar to Nerve Muscle Physiology injury and regeneration
Similar to Nerve Muscle Physiology injury and regeneration (20)
Recently uploaded
Recently uploaded (20)
Nerve Muscle Physiology injury and regeneration
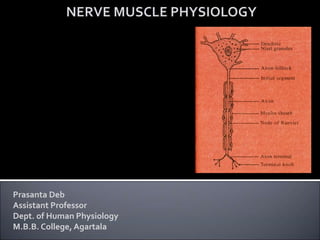
- 1. Prasanta Deb Assistant Professor Dept. of Human Physiology M.B.B. College,Agartala
- 2. P.Deb 2
- 3. Degeneration : After complete transaction of the nerve, the peripheral parts of the axons undergo certain degenerative changes which are often called Wallerian degeneration. Degeneration takes place at three levels : •In the nerve cell •In the proximal part of the cut fibre and •In the distal part of the cut fibre Degeneration : Change occurring in the proximal part of the axons and also the cell bodies following section of an axon is known as retrograde degeneration. The changes in the cell bodies are : 1. Chromatolysis : Nissl granules disappear. It starts within 48 hours and becomes maximum by 15-20 days. 2. Golgi apparatus, mitochondria and neurofibrils break up and disappear. 3. The cell draws in more fluid, swells up and becomes rounded. 3 P.Deb
- 4. 4. The nucleus is pushed to the periphery. In severe cases it may be totally extruded, in which case, the nerve cell completely dies and disappears. The degree of damage and chromatolysis depend on : a) The distance of lesions from the nerve cell- Lesser the distance greater will be the damage. b) Nature of Section : If it is a sharp cut, the effects will be less. But if forcibly torn, the damage is severe and often the cell dies. Degeneration in the Proximal part of the cut fibre Since this part remains connected with the mother cell, degeneration cannot be complete unless the nerve cell dies. Ordinarily, degeneration proceeds centrally as far as upto the first node of Ranvier and in most cases degenerative changes may extend up to a few internodes when regenerative changes are initiated from the end of the central stump. In more severe cases, it may proceed to a little higher. The nature of this degeneration and the subsequent regeneration is same as in the distal stump or part. Regeneration takes place if the neurone survives. 4 P.Deb
- 5. Degeneration in the distal part of the cut fibre Since this part is totally separated from the mother cell, it degenerates completely. Degeneration starts simultaneously in the whole length of the fibre up to its terminal arborizations within 24 hours and is completed by 3 weeks. Following degenerative changes are seen : Histological Changes : 1. The neurofibrils swell, become tortuous and ultimately disappear and the axis cylinder breaks up into short lengths. 2. The myelin sheath disintegrates into droplets of fat. Lecithin splits up into glycerol, phosphoric acid, fatty acid and choline. They are partly removed by macrophages and partly washed out in the blood stream. If the damage be inside the central nervous system, no further change takes place. But if it be in the peripheral nervous system the neurolemma shows the following changes : 5 P.Deb
- 6. The nuclei of Schwann cell multiply mitotically and the Schwann cell cytoplasm increases in amount. It starts 4-9 days after section. The macrophages penetrate the neurolemmal tubes and remove the debris. The Schwann tissue gradually fill up the whole tube and the process is completed by three months. From the cut of the distal end, the proliferating Schwann tissue spreads upwards toward the central cut end and in this way may bridge up a considerable gap (even up to 3 cm) between the two cut ends. The rate of progress of this growth is 1-2 mm per day. The peripheral neurolemmal tube shrinks to half its original diameter in 7 weeks and may remain so for about 18 months. The above degenerative changes in the distal cut end of the fibres were first observed by Waller and according to him it is known as Wallerian degeneration. Degeneration of Nerve endings : The framework of both sensory and motor endings can resist degeneration for months. If the nerve fibre fail to regenerate, the endings also atrophy. Transneuronal degeneration : When neurone or its motor fibre degenerates, the neurone next in the chain is often found to degenerate also. This takes place in spite of the fact that there is no anatomical continuity through the synapses. 6 P.Deb
- 7. It is probably an example of disuse atrophy. In many conditions, this type of degeneration occurs e.g., 1. After section of the optic nerve, the cells in the lateral geniculate body degenerate. 2. After section of the posterior spinal root, the posterior horn cells degenerate. 3. In lesions of the motor cortex or pyramidal tracts, the anterior horn cells may degenerate. This type of degeneration may be the underlying cause of the so-called System diseases viz., Amyotorphic lateral sclerosis, etc., where degeneration of anterior horn cells follows that of the pyramidal tracts. 7 P.Deb
- 8. Regeneration : Regeneration takes place only outside the central nervous system where neurolemma is present. Presence of neurolemma is, therefore, essential for the process. Hence, in the central nervous system, neurolemma being absent, nerve fibre do not regenerate at all. The following steps are seen during regeneration : The axis cylinder grows from the central cut end as a rounded sprout and proceeds towards the solid neurolemmal cord. The proliferated Schwann tissue in the peripheral cut end and its prolongation towards the central cut end provide an influence which guides the approaching axis cylinder. Each growing fibre splits up into numerous neurofibrils (even up to 100), the Schwann cells disappear and the fibrils enter the newly made neurolemmal tube (2-3weeks after the section, the inner wall of the tube may contain a number of fibrils). All the fibrils degenerate, excepting a single one, which gradually enlarges and occupies the central part of the whole length of the tube proceeding peripherally. The daily rate of growth is about 0.25 mm in the scar tissue between the two cut ends and 3-4 mm in the peripheral neurolemmal tubes. 8 P.Deb
- 9. Myelin sheath begins to appear in about 15 days and proceeds peripherally along the fibre at a slower rate than the growing axis cylinder. Increase in the diameter of the fibre takes place slowly. The diameter of the fibre is limited by the size of the neurolemmal tube and that of the parent nerve cell. With a clean sharp wound and the cut ends being in apposition, some degree of recovery usually takes place in 6-24 months. For a motor nerve, recovery may be complete. But for a mixed nerve, it is rarely so. In the regenerated fibres the axis cylinder and myelin sheath are reduced in thickness, the intermodal distance is also diminished. But the rate of conduction of nerve impulses in the regenerated fibres remains the same. Complete functional regeneration occurs after histological regeneration- 3 weeks in case of motor nerve fibres and 5 weeks in case of sensory nerve fibres. 9 P.Deb
- 10. P.Deb 10
- 11. P.Deb 11 Modern concept of Generation of Resting Potential
- 12. P.Deb 12 Resting membrane potential (RMP) is the difference between electrical potential existing on the outside and inside of a cell at rest. This varies in different types of cells. In a nerve, usually it is -70 mV. In a skeletal muscle, it is about -90 mV. In intestinal smooth muscle, it is about -50mV. Cause of Resting Membrane Potential : The intracellular and extracellular concentration of ions such as Na+, K+,Cl- are different. Also, the permeability of cell membrane to the individual ions is also different. These two factors are mainly responsible for the magnitude of RMP. [K+] inside the cell is 155 meq/L and [K+] outside the cell is 4 meq/L. As the cell membrane is freely permeable to K+ ions, K+ tends to move out of the cell along the concentration gradient. But as K+ moves out of the cell, the interior of the cell becomes negatively charged due to loss of cations. This could have been prevented- a. If Na+ ions entered in to the cell but the cell membrane is impermeable to Na+ ions.
- 13. P.Deb 13 b. Proteins anions inside the cells could have moved out to neutralise intracellular negativity but they are too large to pass through the cell membrane. c. Cl- ions also cannot move out of the cell against the steep concentration gradient. So, intracellular negativity persists. This will attract the outgoing positively charged K+ ions inwards due to electrical gradient. At a particular electrical potential, these two forces due to concentration and electrical gradient balance each other and an equilibrium is established. This is known as the diffusion or equilibrium potential of K+. This can be mathematically derived from Nernst equation, according to which RT [K+]0 EK = ------------ln _______ FZ [K+]I
- 14. P.Deb 14 Where, EK= Equilibrium potential of K+ ions R= Gas Constant T= Absolute temperature F= Faraday (96500 Coulombs) Z= Valency of K+ ln= Natural log [K+]0= K+ concentration outside the cell [K+]I= K+ concentration inside the cell In contrast to K+ ions, Na+ ions have electrical gradient and concentration gradient both directed to the inside of the cell. From the Nearst equation, we get ENa=+65 mV Similarly, ECl= -70mV
- 15. P.Deb 15 So, K+ ions tend to move the RMP to its equilibrium potential (EK) i.e., -90mV, whereas Na+ ions tend to pull the RMP in the opposite direction to ENa + , which is +65mV. Similarly Cl- ions try to maintain the RMP at its own equilibrium potential which is -70mV. Cl- ions have a tendency to move out of the cell being repelled by the electronegative cell interior whereas it has a tendency to move into the cell due to concentration gradient directed towards inside of the cell. Normally, these two opposite tendencies almost exactly balance each other and Cl- ion has very little effect on RMP. The resultant RMP now depends on the permeability or conductance of the individual ions. As the K+ ions is 10-25 times more permeable than Na+ ion, the resting membrane potential is much closer to EK. Actual RMP stands at -70 mV. It can be mathematically derived from the Goldman constant-field equation.
- 16. P.Deb 16 RT PK[K+]o+PNa[Na+]o+PCl[Cl-]i RMP = ln F PK[K+]i+PNa[Na+]i+PCl[Cl-]o Where, P stands for permeability, ‘o’ and ‘I’ stand for outside and inside respectively and third brackets indicate concentration.
- 17. P.Deb 17 It is to be noted that at RMP, neither K+ ions nor Na+ ions are at their equilibrium potential. So, there is movement of Na+ ions into the cell and K+ ions out of the cell. However, this does not alter the intracellular or extracellular Na+ and K+ ion concentrations as Na+-K+-ATPase pumps constantly pump out Na+ out of the cell and bring K+ into the cell, thus restoring ionic balance. A small part of the RMP is contributed directly by the electrogenic Na+-K+- ATPase pump, as it drives out 3 Na+ ions from the cell and brings 2K+ ions into the cell, thus causing slight intracellular negativity. Although, the direct contribution of Na+-K+-ATPase pump to RMP is small, it has a far more important indirect role in the genesis of RMP as it plays a pivotal role in maintaining concentration gradients of Na+ and K+ ions across the cell membrane. Donnan membrane equilibrium results in unequal distributions of anions and cations across the cell membrane due to the presence of non-diffusible anions (Proteins) as a result an electrical potential difference is set up in accordance with Nernst equation.
- 18. P.Deb 18 GENERATION OF ACTION POTENTIAL
- 19. P.Deb 19 In resting state the nerve fibre remains in polarized state and the membrane potential lies within -70 mV. The inside of the nerve is negative and the outside of the nerve is positive. Na+ concentration outside the membrane is higher than that of inside the membrane. K+ concentration inside the membrane is also higher than that of the outside. K+ can permeate through the membrane at resting state but Na+ cannot permeate. Permeability of Na+ to membrane is increased only after excitation and is the first event of the action potential. The action potential occurs in successive stages of depolarization, repolarization, negative after potential and positive after potential. It has been postulated that in resting state calcium ions (Ca++) remain bound to the protein through these resting pores. During excitation Ca++ is dislodged from its binding site and the permeability to Na+ is increased. So the depolarization starts with the onset of Na+ entry and thus an increase in Na+ conductance is taken place.
- 20. P.Deb 20
- 21. P.Deb 21
- 22. P.Deb 22 The tremendous increase in Na+ conductance during this period is known as activation of membrane. Due to this, the reversal of potential is caused with the development of positivity inside the membrane and negativity outside . But with the increase of positivity inside, further entry of Na+ is prevented and calcium begins to bind with the proteins of the membrane pores. But as soon as the action potential attains the voltage approximately +35 mV, K+ begins to come out from inside the membrane. The inside becomes negative and outside becomes positive again. This stage is the repolarization phase, K+ conductance is increased to the maximum. The mechanism underlying the process of K+ conductance is mostly hypothetical and increased positivity inside the membrane due to Na+ entry during depolarization phase, allows the K+ to come out and the resting potential is slowly achieved. But at the later period of this phase (at the termination of spike potential) K+ conductance is allowed down and thus a few milliseconds are delayed in restoring the membrane potential. This state is known as negative after potential which has been described to be the cause of increased K+ concentration outside the membrane.
- 23. P.Deb 23 With the disappearance of the negative-after potential, though the resting membrane potential is achieved yet the resting ionic status is not established. It is achieved by the active Na+ pump mechanism and Na+ begins to come out from inside the membrane creating negativity again. The positive after potential is due to this process of Na+ diffusion from inside to outside the membrane. The negativity produced due to active Na+ pump mechanism, causes the K+ to diffuse back to the interior of the nerve fibre. For the active Na+ and K+ pump mechanism high energy phosphate (ATP) is required. In this way resting normal ionic status is established during the period of positive-after potential.
- 24. P.Deb 24
- 25. P.Deb 25 PROPERTIES OF SYNAPSE 1. ONEWAY CONDUCTION (BELL-MAGENDIE LAW) According to Bell-Magendie law, the impulses are transmitted only in one direction in synapse, i.e. from presynaptic neuron to postsynaptic neuron. 2. THE SYNAPTIC DELAY During the transmission of impulses via the synapse, there is a short delay in transmission. It is called the synaptic delay. It is due to the time taken for : i. Release of neurotransmitter ii. Movement of neurotransmitter from axon terminal to post synaptic membrane. iii. Action of the neurotransmitter to open the ionic channels in post synaptic membrane. The synaptic delay is one of the causes for the latent period of the reflex activity.
- 26. P.Deb 26 3. FATIGUE During continuous muscular activity, the synapse forms the seat of fatigue along with the Betz cells present in the motor area of the frontal lobe of the cerebral cortex. The fatigue at the synapse is due to the depletion of neurotransmitter substance, acetylcholine. Depletion of acetylcholine occurs by two factors : i. Soon after the action, acetylcholine is destroyed by acetylcholinesterase. ii. Due to continuous action, new acetylcholine is not synthesized. These two factors leads to lack of acetylcholine resulting in fatigue. 4. SUMMATION When many presynaptic excitatory terminals are stimulated simultaneously or when single presynaptic terminal is stimulated repeatedly, there is summation or fusion of effects in postsynaptic neuron, i.e. there is progressive increase in the excitatory postsynaptic potential. It is called summation. Summation is of two types :
- 27. P.Deb 27 i. Spatial Summation : It occurs when many presynaptic terminals are stimulated simultaneously. ii.Temporal Summation : It occurs when one presynaptic terminal is stimulated repeatedly. Thus, both spatial summation and temporal summation play an important role in the facilitation of response. 5. ELECTRICAL PROPERTY The electrical properties of synapse are the EPSP and IPSP. When action potential causes increased permeability of the postsynaptic membrane to all ions viz., Na+, K+ and Cl-, then it results in EPSP (Excitatory post synaptic potential) When action potential causes selective permeability of the postsynaptic membrane to K+ ions, then it results in IPSP (Inhibitory post synaptic potential)
- 29. P.Deb 29 The skeletal muscle fibres are innervated by large, myelinnated nerve fibres that originate from large motor neurons in the anterior horns of the spinal cord. Each nerve ending make a junction, called the neuromuscular junction, with the muscle fibre near its midpoint. The action potential initiated in the muscle fibre by the nerve signals travels in both directions toward the muscle fibre ends. Physiologic anatomy of the neuromuscular junction- The motor end plate The neuromuscular junction form a large, myelinated nerve fibre to a skeletal muscle fibre. The nerve fibre forms a complex of branching nerve terminals that invaginate into the surface of the muscle fibre but lie outside the muscle fibre plasma membrane. The entire structure is called the motor end plate. It is covered by one or more Schwann cells that insulate it from the surroundings fluids. The invaginated membrane of the muscle fibre membrane is called the synaptic gutter or synaptic trough.
- 30. P.Deb 30 The space between the terminal and the fibre membrane is called the synaptic space or synaptic cleft. This space is 20-30 nm wide. At the bottom of the gutter are numerous smaller folds of the muscle membrane called subneural clefts, which greatly increase the surface area at which the synaptic transmitter can act. In the axon terminal numerous mitochondria supply ATP for the synthesis of neurotransmitter acetylcholine. The acetylcholine inturn excites the muscle fibre membrane. Acetylcholine is synthesized in the cytoplasm of axon terminals but are absorbed rapidly in to many small synaptic vesicles about 300,000 in the terminal of a single end plate. In the synaptic space are large quantities of the enzyme acetylcholine esterase, which destroys acetylcholine in a few milliseconds after it has been released from the synaptic vesicles.
- 31. P.Deb 31 Mechanism of transmission of nerve impulse across the neuromuscular junction When a nerve impulse reaches the neuromuscular junction, about 125 vesicles of acetylcholine is released from the terminals into the synaptic space. On the inside surface of the neural membrane are linear dense bars. To each side of each dense bar are protein particles that penetrate the neural membrane, these are voltage gated calcium channels. When action potential spreads over the terminals, these channels open and allow calcium ions to diffuse from the synaptic space to the interior of the nerve terminal. The calcium ions, in turn, are believed to exert an attractive influence on the acetylcholine vesicles, drawing them to the neural membrane adjacent to the dense bars. The vesicles then fuse with the neural membrane and empty their acetylcholine into the synaptic space by the process of exocytosis. At the neck of the subneural clefts there exists the acetylcholine receptors in the muscle fibre membrane.
- 32. P.Deb 32
- 33. P.Deb 33 These are acetylcholine-gated ion channels, and they are located almost entirely near the mouths of the subneural clefts lying immediately below the dense bar areas, where acetylcholine is emptied into the synaptic space. The receptor is a protein complex(MW-275,000), the complex is composed of five subunits proteins, two alpha proteins and one each of beta, delta, and gamma proteins. These protein molecules penetrate all the way through the membrane , lying side by side in a circle to form a tubular channel. The channel remains constricted until two acetylcholine molecules attach respectively to the two alpha subunit proteins . This causes a conformational change that opens the channel. The opened acetylcholine channel has a diameter of 0.65 nm, which is large enough to allow the important positive ions – Na+, K+ and Ca++ to move easily through the opening.
- 34. P.Deb 34
- 35. P.Deb 35 Whereas the negative ions such as Cl- ions cannot pass through because of strong negative charges in the mouth of the channel that repel these negative ions. In practice far more Na+ ions move through the acetylcholine channels than any other ions due to two reasons : 1. The extracellular concentration of Na+ ions is more , and 2. The inside is electronegative (-70 to -90mV) which easily allows the Na+ ions to enter and at the same time prevents the efflux of the K+ ions to outside. This creates a local positive potential change inside the muscle fiber membrane, called the end-plate potential. In turn, this end plate potential initiates an action potential that spreads along the muscle membrane and thus causes muscle contraction. The acetylcholine, once released into the synaptic space , continues to activate the acetylcholine receptors as long as the acetylcholine persists in the space.
- 37. P.Deb 37 Acetylcholine is removed by two means- 1. Most of the acetylcholine is destroyed by the acetylcholinesterase enzyme present in the synaptic space remains attached to the fine connective tissues. 2. A small amount of acetylcholine diffuses out of the synaptic space and is then no longer available to act on the muscle fibre membrane.
- 38. P.Deb 38 What is Reflex ? It is the involuntary or autonomic response elicited by specific stimulus of threshold intensity with the involvement of CNS. ReflexArc : It is the pathway through which any reflex action is mediated. The Components of reflex arc are as follows : i. Receptor : This detects the change of internal or external environment and transmits the impulse to center. ii. Afferent (sensory) nerve- It carries the impulse from receptor to center. iii. Higher centers- It is the part of CNS where afferent limb ends and either synapses directly with efferent motor neuron or establish connection with the efferent neuron via interneurones. iv. Efferent (Motor ) nerve- It carries the efferent impulses from the centre to the efferent organ. v. Efferent organ – These are basically muscles or glands which shows the reflex action.
- 39. P.Deb 39 Classification of reflexes : a. Depending on inborn or acquired : It is of two types- i. Unconditioned reflex : These reflexes are present since birth i.e. inborn. Example : Salivation after taking food, knee jerk etc. ii. Conditioned reflex : These are not present from birth but acquired in later life on the basis of past experiences through conditioning and learning. Example : Salivation by seeing tasty food the taste of which is known. b. Depending on the number of synapses present in the reflex arc : It is of two types : i. Monosynaptic reflex : When there is only one synapse present in the reflex arc it is known as monosynaptic reflex. Example : Knee jerk, Ankle jerk etc.
- 40. P.Deb 40 ii. Polysynaptic reflex : When more than one synapse is present in the reflex arc it is known as polysynaptic reflex. Example : Withdrawl reflex i.e., protective reflex e.g. automatic withdrawl of limb if it comes in contact with hot object. C. Physiological Classification : It is of two types : i. Extensor reflex : These reflexes are responsible for extensor movement of limbs at joints. Stretch reflexes are extensor reflexes.These are responsible for muscle tone and posture. ii. Flexor reflexes :These are reflexes which cause flexion of the joints in response to nociceptive (pain) stimuli.Withdrawl reflexes are the example of flexor reflex. D. Functional classification : are of two types- i. Somatic reflex : It involves the somatic nervous system. Example- Knee jerk ii. Autonomic reflex : It involves the autonomic nervous system. Example- Sino-aortic reflex.
- 41. P.Deb 41 E. Clinical Classification : It is of four types : i. Superficial reflexes : These are initiated by stimulating appropriate receptors of skin and mucous membrane. These are usually polysynaptic. Example : Planter reflex, corneal reflex etc. ii. Deep reflexes : These are elicited on stroking the tendon. These are basically stretch reflexes. Example : Knee jerk, ankle jerk etc. iii. Visceral reflexes : These are reflexes in which part of the reflex arc is formed by autonomic nervous system. Example- Papillary reflex, Carotid sinus reflex etc. iv. Pathological reflexes : These are not found normally. Elicited in case of diseased state.
- 42. P.Deb 42
- 43. P.Deb 43
- 44. P.Deb 44
- 45. P.Deb 45
- 46. P.Deb 46
- 47. P.Deb 47
- 48. P.Deb 48 Reflex Action : Reflex action is an involuntary effector response due to a sensory stimulus. It is the basic physiological unit of integration in the neural activity. Unconditioned Reflex : Unconditioned reflexes are inborn. The nerve paths are fixed from the very birth. Any material alteration is considered as disease. Hence, examination of reflexes is a great help in the diagnosis of various diseases. Conditioned Reflex : The conditioned reflexes are acquired after birth. Such reflexes need previous learning, training, or conditioning. The example is the secretion of saliva by the sight, smell, thought or hearing of a known edible substance. Cerebral cortex is responsible for the establishment of conditioned reflexes through the development of new connection with different subcortical centres. For establishment of conditioned response or reflex through specific
- 49. P.Deb 49 conditioned stimuli, specific cortical and subcortical centres are responsible for its development. As for example, for the production of conditioned salivation reflexes, the cortical taste centres as well as the visual and auditory areas along with its subcortical centres are responsible if the conditioned stimulus are the ringing of bell and giving of food.