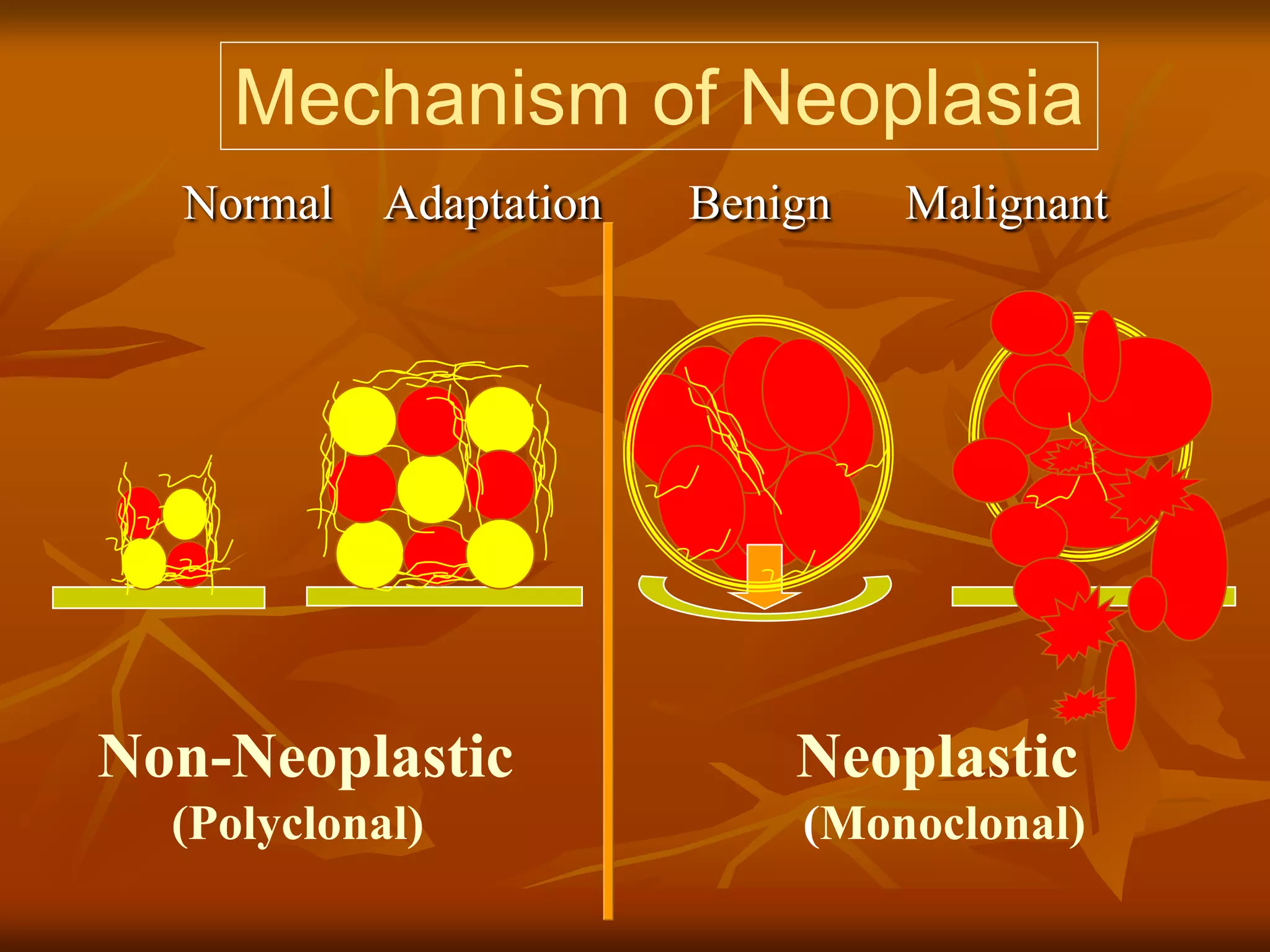

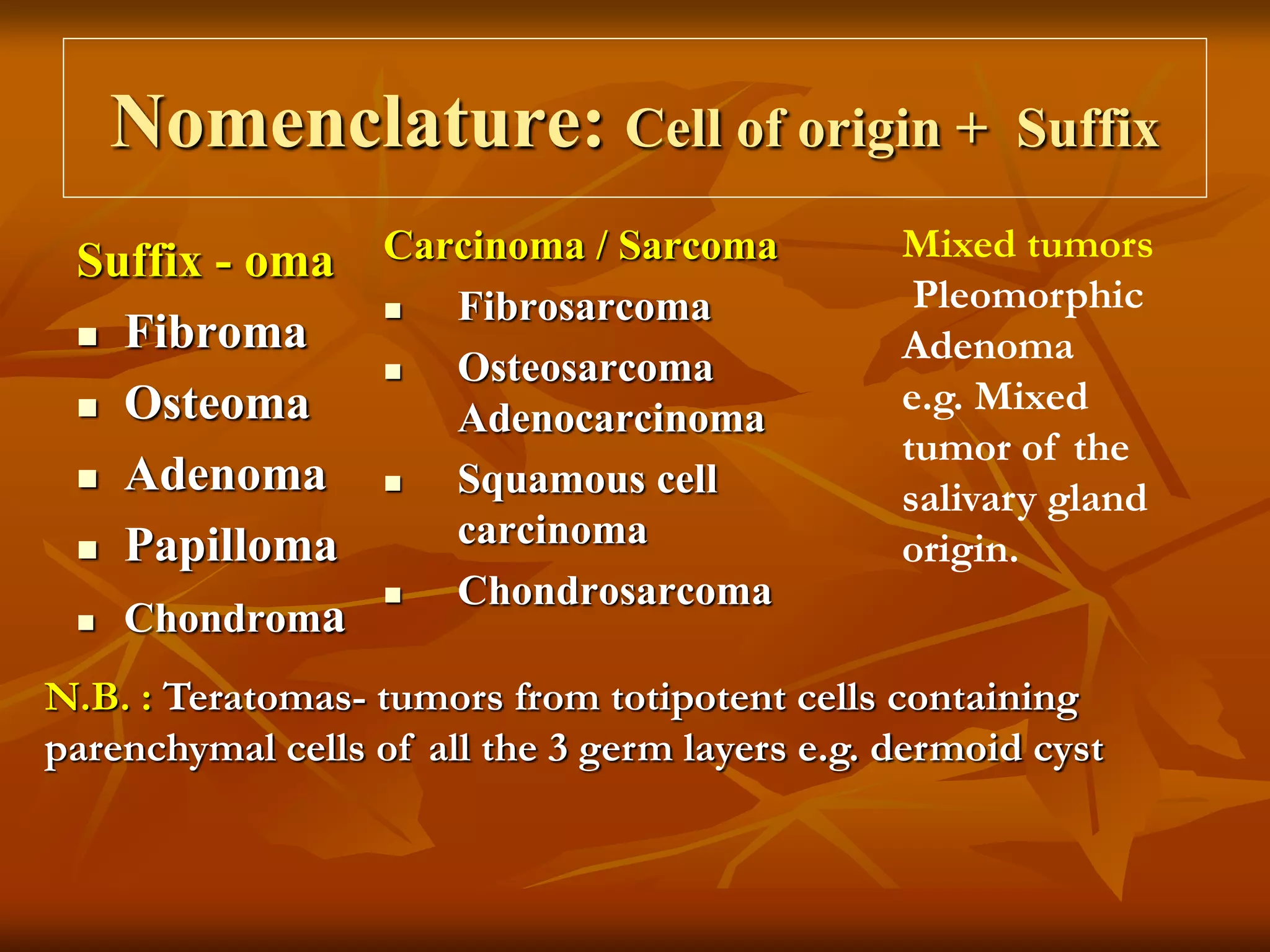
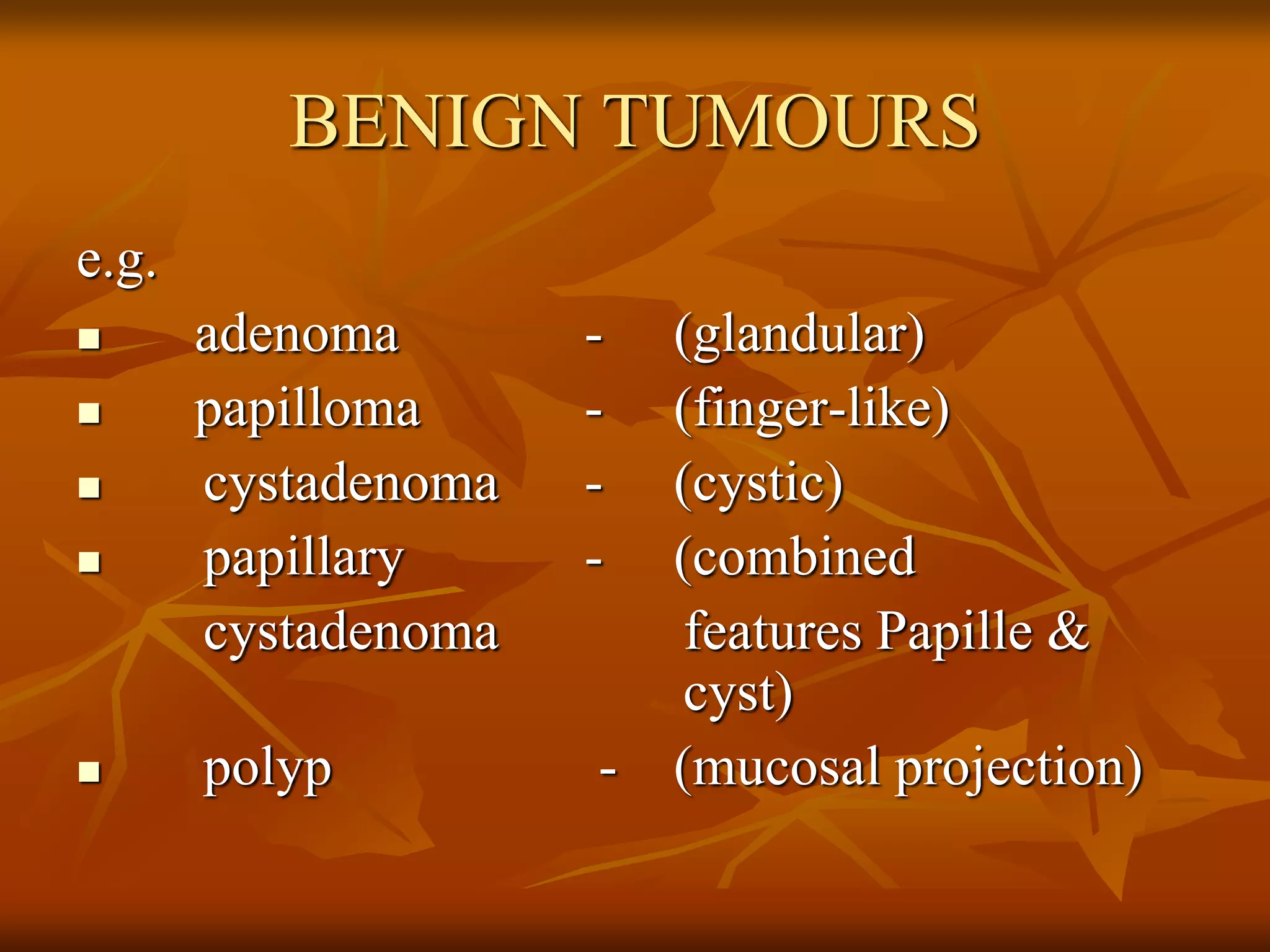













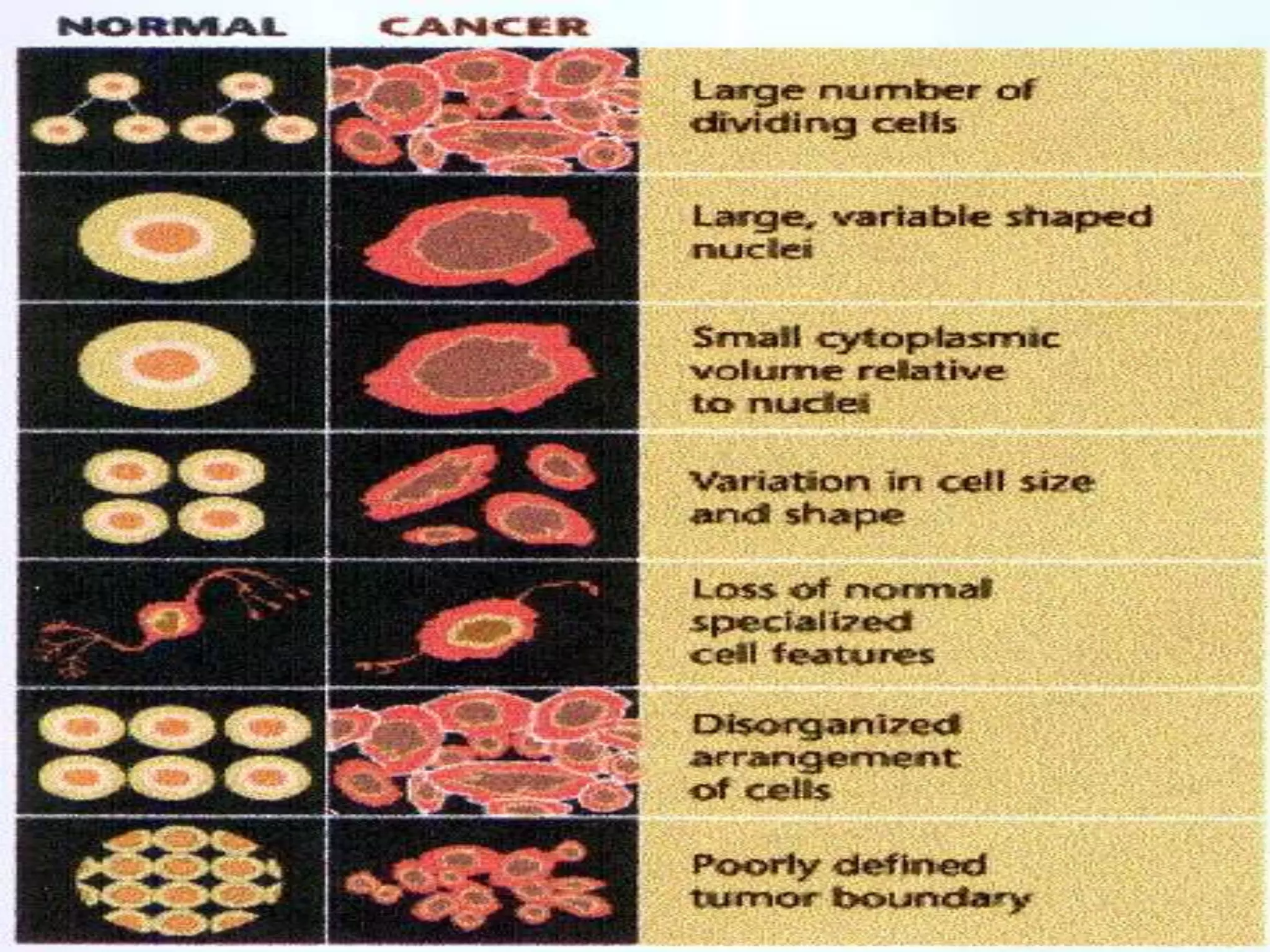


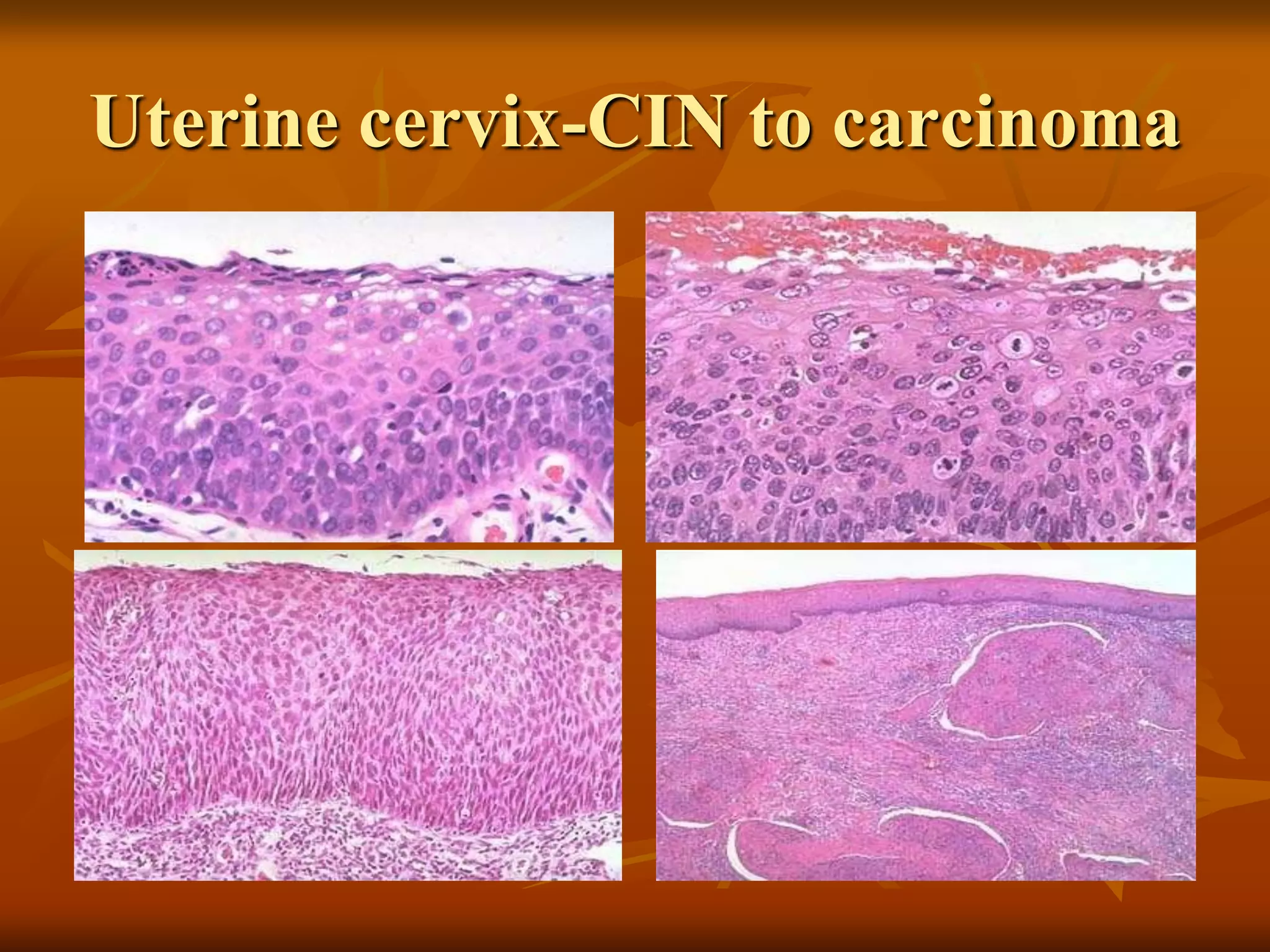

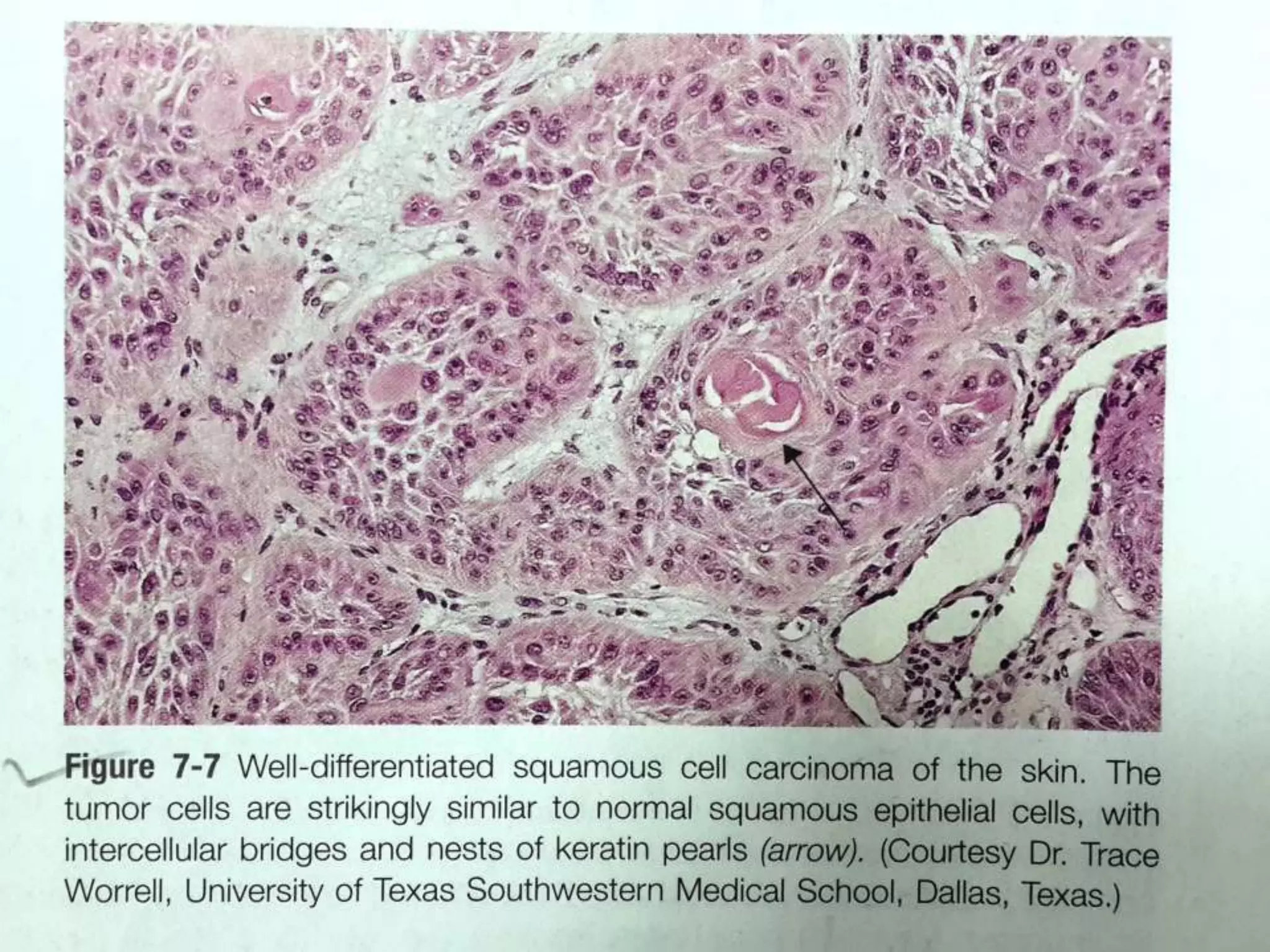


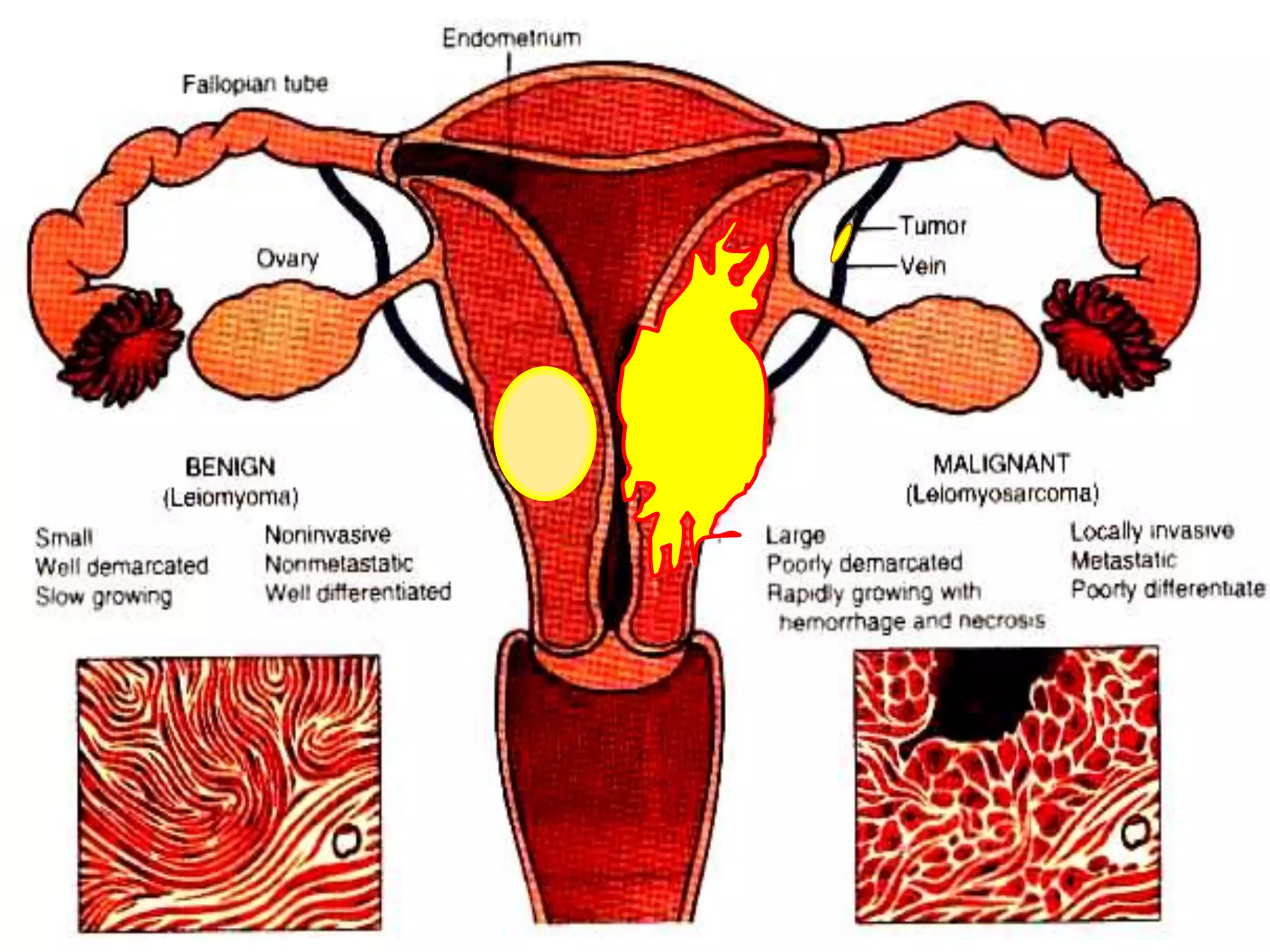














This document discusses the terminology and classification of tumors (neoplasms). It begins by defining key terms like neoplasia, oncology, and cancer. It describes Dr. Willis' definition of a neoplasm and explains that neoplasms differ from normal tissue in growth, differentiation, function, and organization. Benign tumors are distinguished from malignant tumors based on features like differentiation, growth rate, invasion, and metastasis potential. The document provides examples of benign and malignant tumor types based on cell of origin. It also covers tumor nomenclature conventions and histopathological grading of tumors from well-differentiated to anaplastic.

![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)