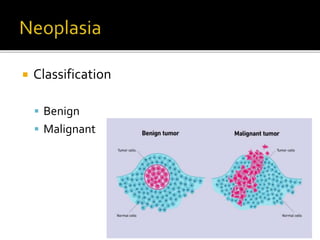
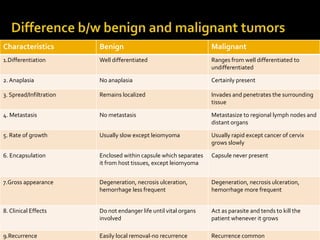
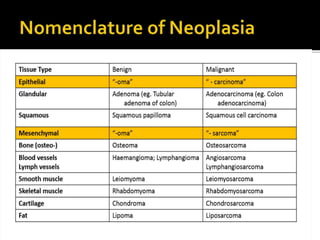
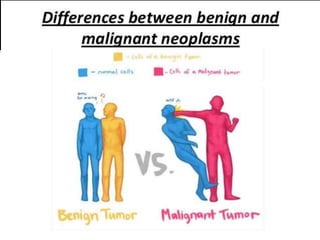
Cancer is a leading cause of death characterized by abnormal cell proliferation resulting in neoplasms, which can be benign or malignant. Benign tumors remain localized and do not metastasize, while malignant tumors invade surrounding tissues and can spread to distant organs. The document discusses the classifications, characteristics, nomenclature, and biological behavior of various types of tumors, as well as the process of metastasis.















































![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)






























