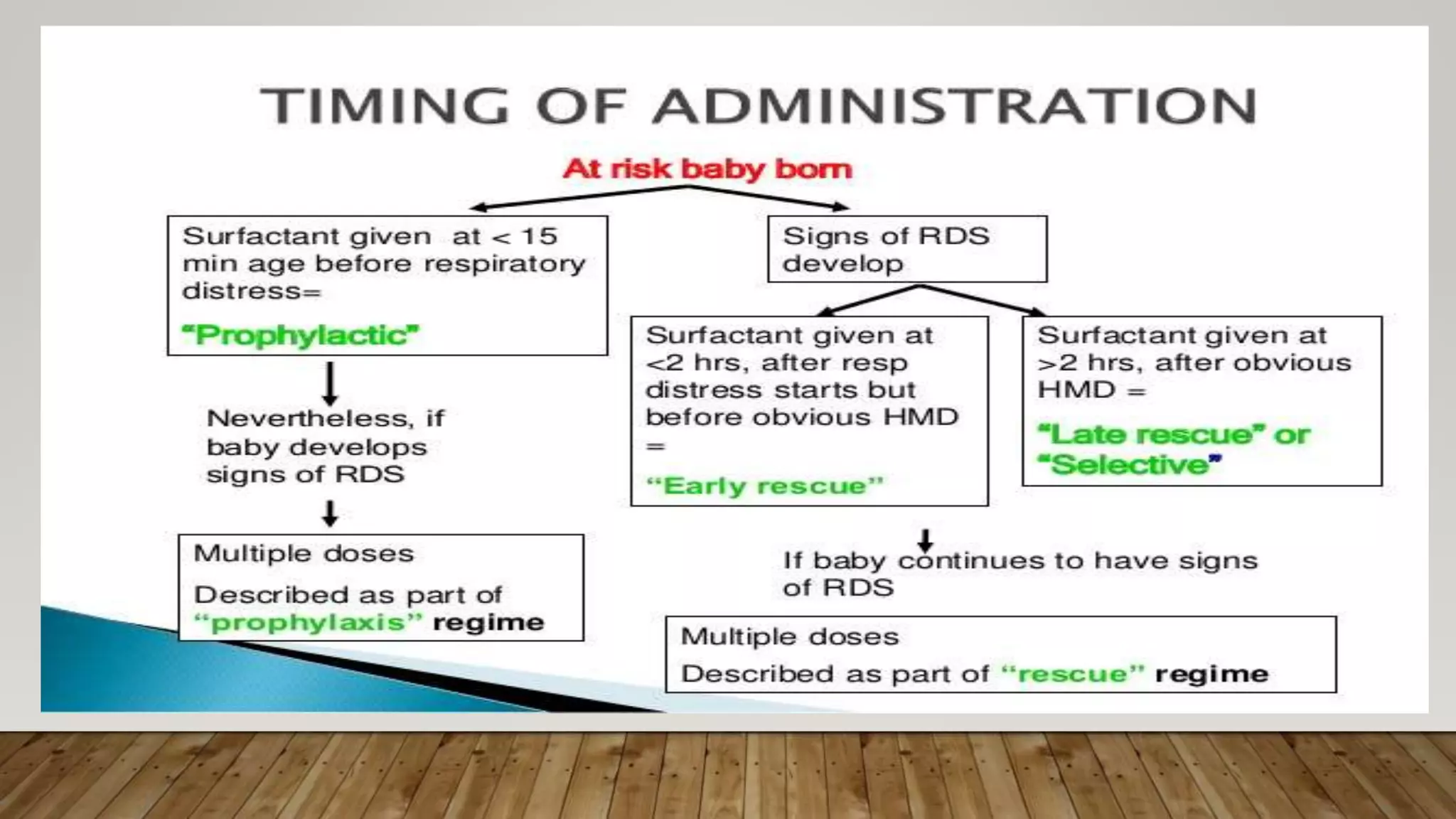
Surfactant therapy is a crucial treatment for preterm infants with respiratory distress syndrome (RDS) caused by surfactant deficiency, first identified in 1959. This therapy can reduce mortality and improve outcomes for these infants, with natural surfactants showing superior results over synthetic alternatives. Early initiation of surfactant treatment, especially within the first two hours of life, significantly decreases risks associated with RDS, including mortality and chronic lung disease.