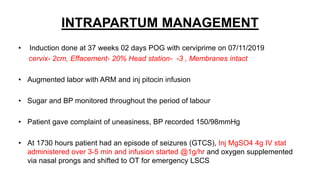
Mrs. Guddan, a 34-year-old patient with a history of gestational diabetes and pre-eclampsia, was admitted at 36 weeks and 5 days for monitoring and early termination of pregnancy. Induction was performed at 37 weeks and 2 days due to complications, including hypertension and seizures, leading to an emergency cesarean section and the birth of a healthy male infant. Post-operative care included monitoring in ICU and management of maternal hypertension and diabetes-related concerns.