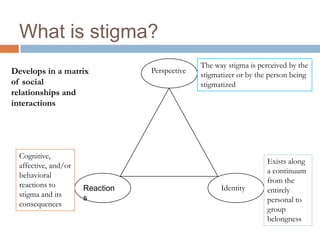
This document discusses stigma related to mental illness. It begins by defining stigma as prejudices related to having a mental illness, as coined by Goffman. Throughout history, madness has been seen as a perverted will or symptoms of animal instincts. The document then discusses the stigma faced by the character Hester in The Scarlet Letter, who is forced to wear a badge of humiliation but refuses to let others determine her identity. Key aspects of stigma are discussed, including its visible, controllable, and impactful nature. Public stigma impacts life goals like employment and independence, while self-stigma causes social isolation and low self-esteem. Changing stigma requires targeted approaches like contact-based programs and addressing discriminatory attitudes and behaviors