




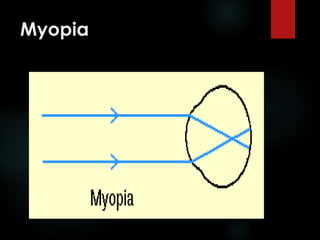

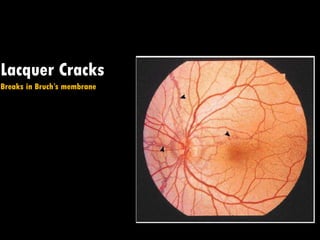
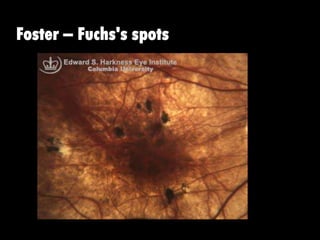
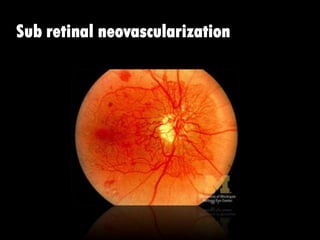
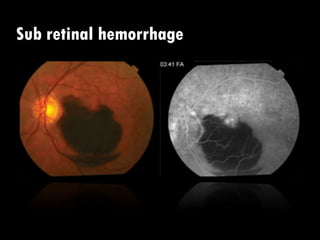
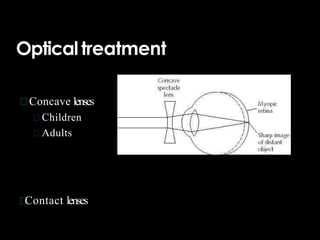


This document discusses myopia (nearsightedness) including its causes, classifications, signs and symptoms, and treatment options. Myopia occurs when the eyeball is too long or the refractive power is too strong for the eye length, causing light to focus in front of the retina. It is classified based on progression rate, anatomy, degree, age of onset, and whether it involves degenerative changes. Symptoms include blurred distant vision. Treatment includes optical correction with glasses or contacts and refractive surgery procedures like LASIK. Advanced myopia can lead to retinal damage and complications like detachment.





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
