Download to read offline



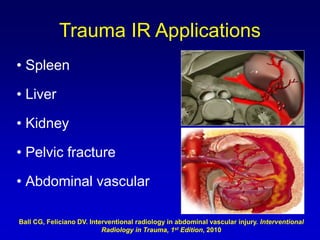
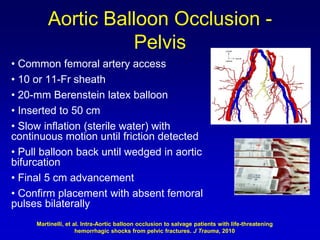
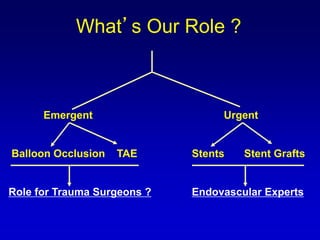
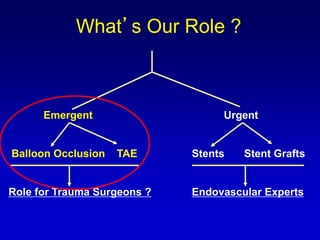

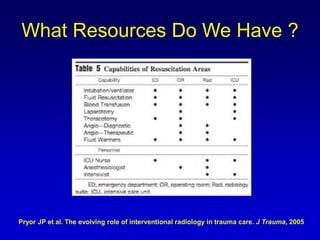
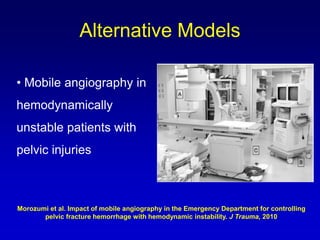

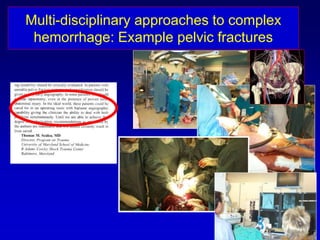

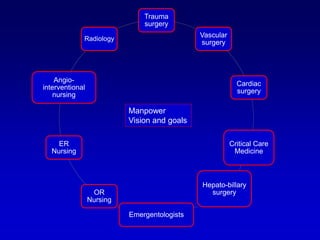
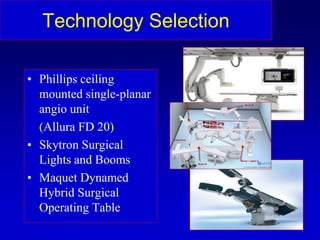
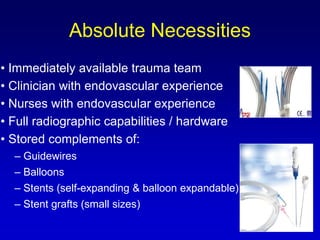
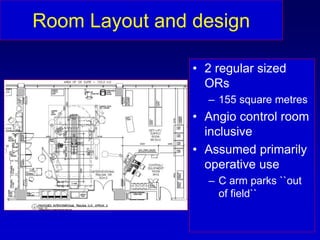





This document discusses hybrid operating theaters/environments for treating hemorrhage in trauma patients. It provides an overview of endovascular techniques like transcatheter arterial embolization and balloon occlusion that can be used to treat hemorrhage. Trauma applications like treatment of spleen, liver, kidney and pelvic fractures are mentioned. The role of trauma surgeons working with interventional radiologists is discussed. The document also describes the process of developing a hybrid operating room called RAPTOR at a hospital in Canada, including securing funding, designing the space, and implementing protocols for its use. An analysis found it benefited around 6% of severely injured patients with persistent hemorrhage.























































































