Download to read offline
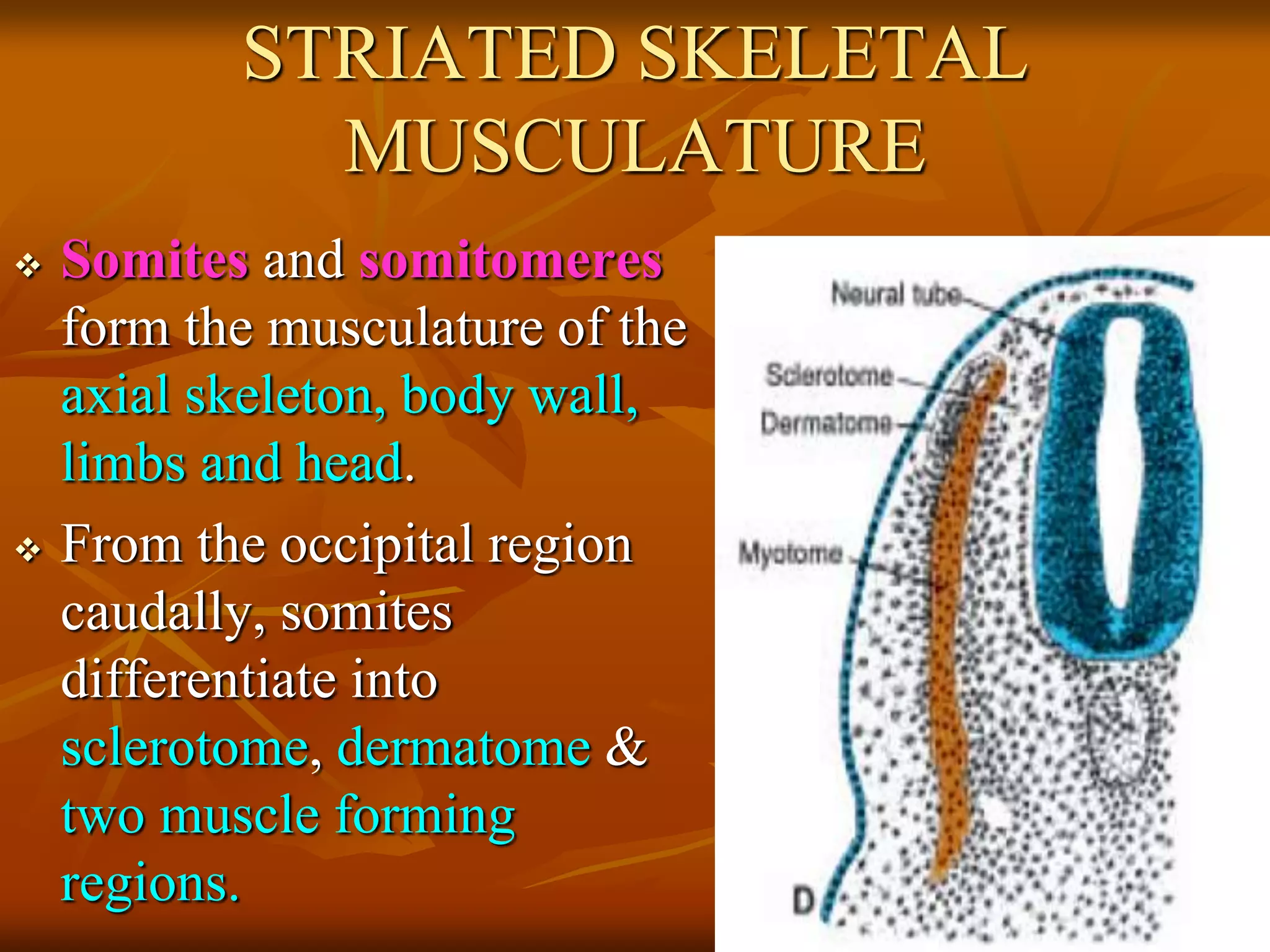
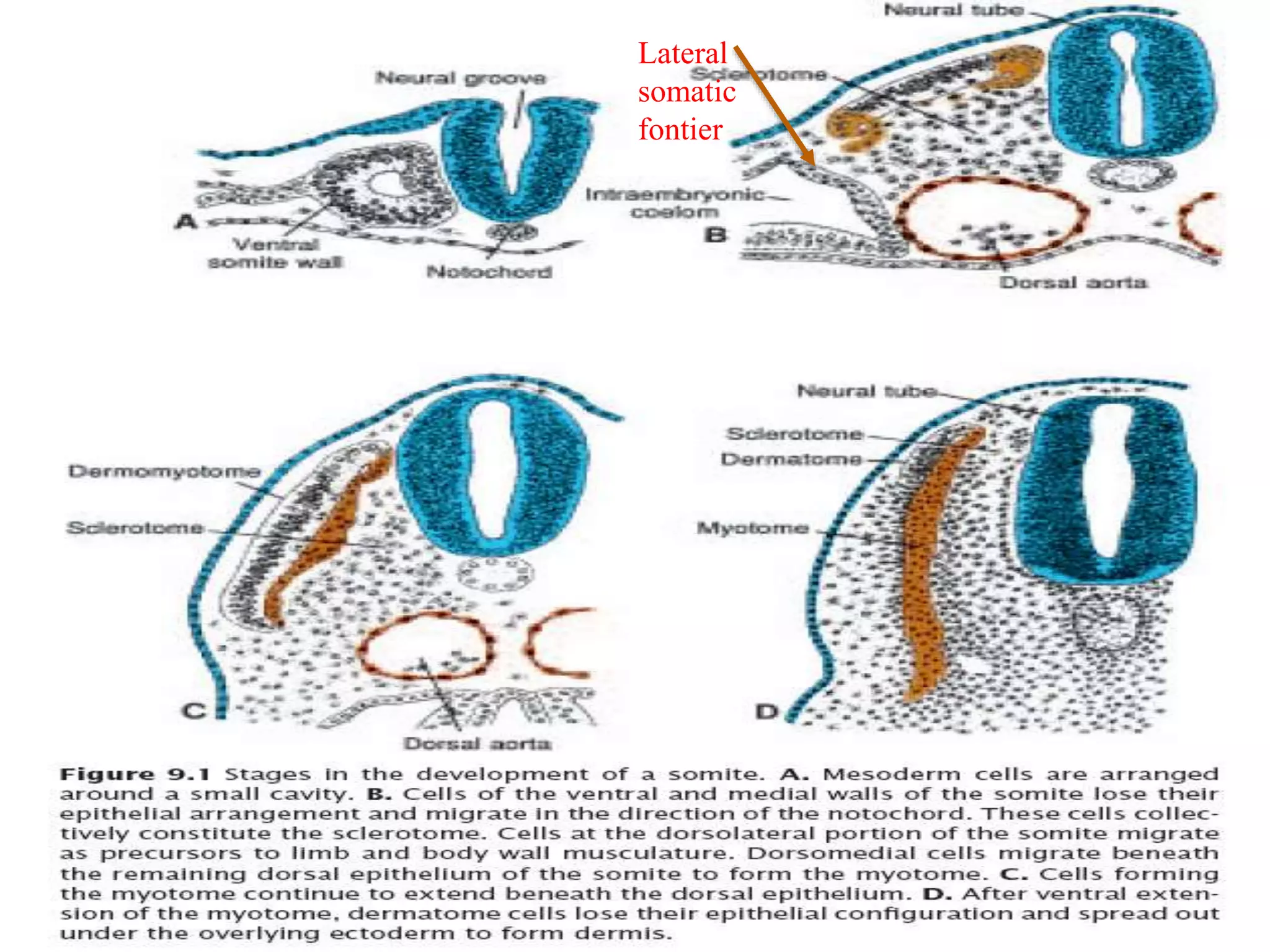
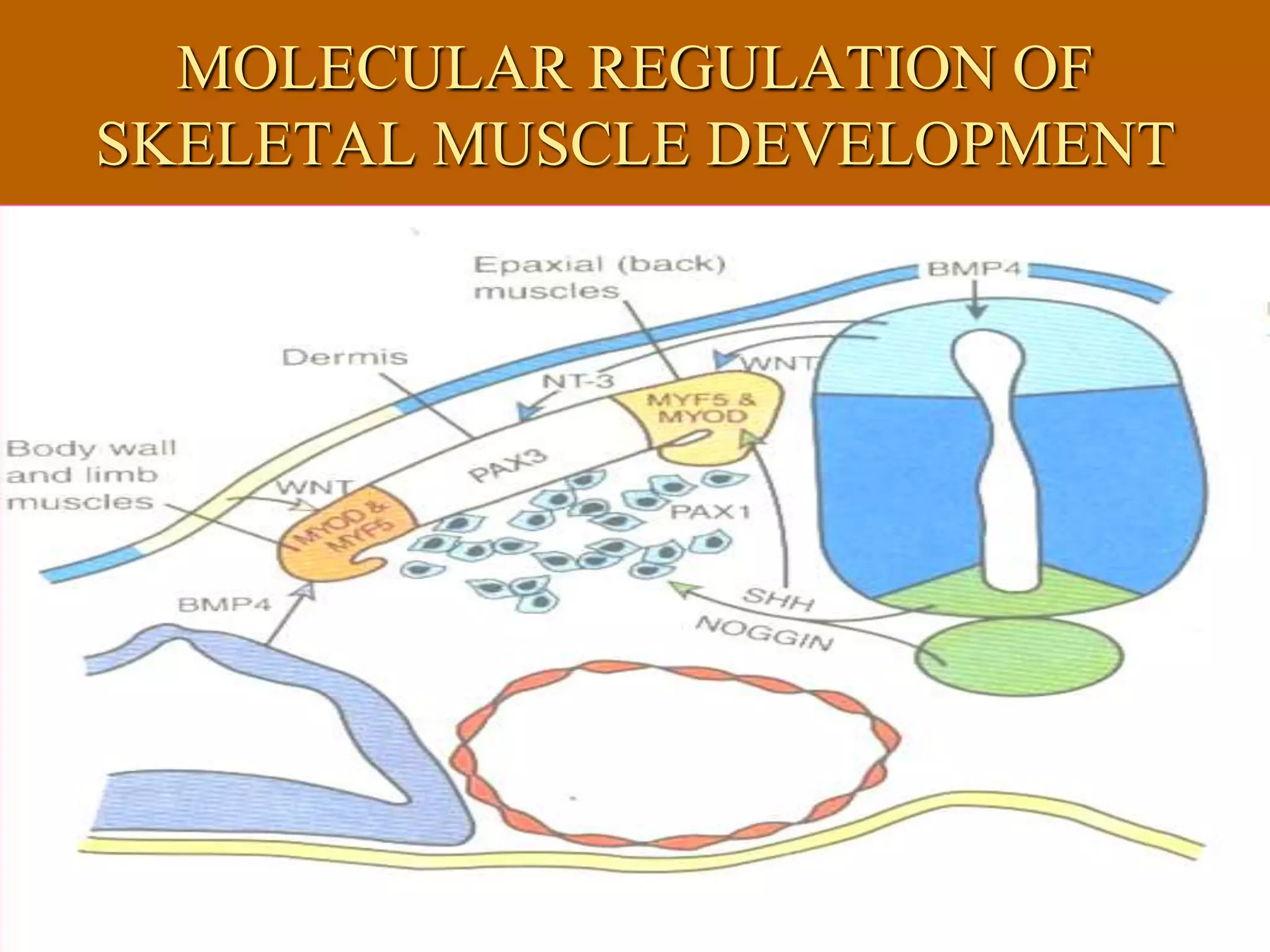




The muscular system develops primarily from the mesodermal germ layer. It consists of skeletal, smooth, and cardiac muscle. Skeletal muscle develops from paraxial mesoderm and forms the musculature of the axial skeleton, body wall, and limbs. Smooth muscle develops from splanchnic mesoderm surrounding organs and the ectoderm of certain structures. Cardiac muscle develops from splanchnic mesoderm surrounding the heart tube. Muscle tissue develops from embryonic muscle cells called myoblasts that fuse to form long muscle fibers containing myofibrils. Precise molecular signaling regulates the development of each muscle type from precursor tissues and cells.
![Development of the Muscular System [Human Embryology]](https://cdn.slidesharecdn.com/ss_thumbnails/developmentofthemuscularsystemhumanembryology-190416145251-thumbnail.jpg?width=640&height=640&fit=bounds)


































































