Download to read offline


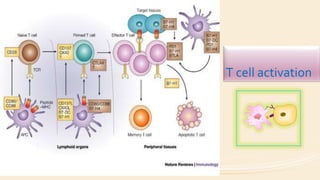
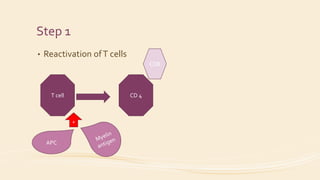
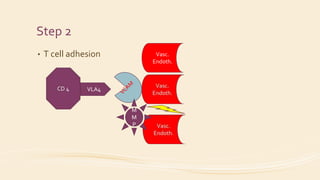
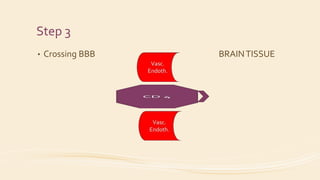

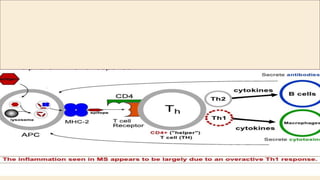
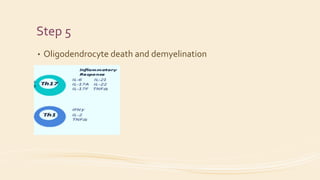
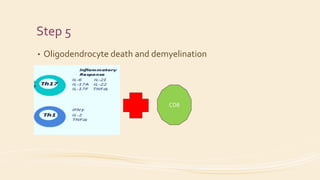
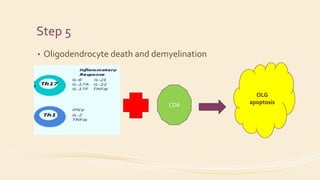

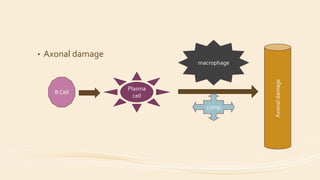



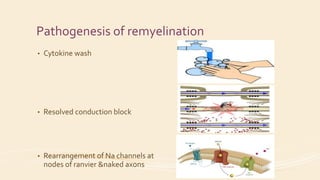
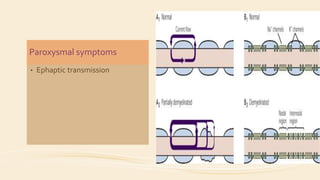



Multiple sclerosis is caused by an immune-mediated process where activated T cells are reactivated and cross the blood-brain barrier. This leads to oligodendrocyte death and demyelination through cytokines and macrophage activity. Axonal damage can also occur through antibodies, complement activation, and oxidative stress. Symptoms are caused by disrupted conduction in partially demyelinated axons. Remyelination involves cytokine clearance and axonal rearrangement at nodes of Ranvier. Some aspects of pathogenesis remain enigmatic, such as clinically silent lesions and symptom production without demyelination.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







