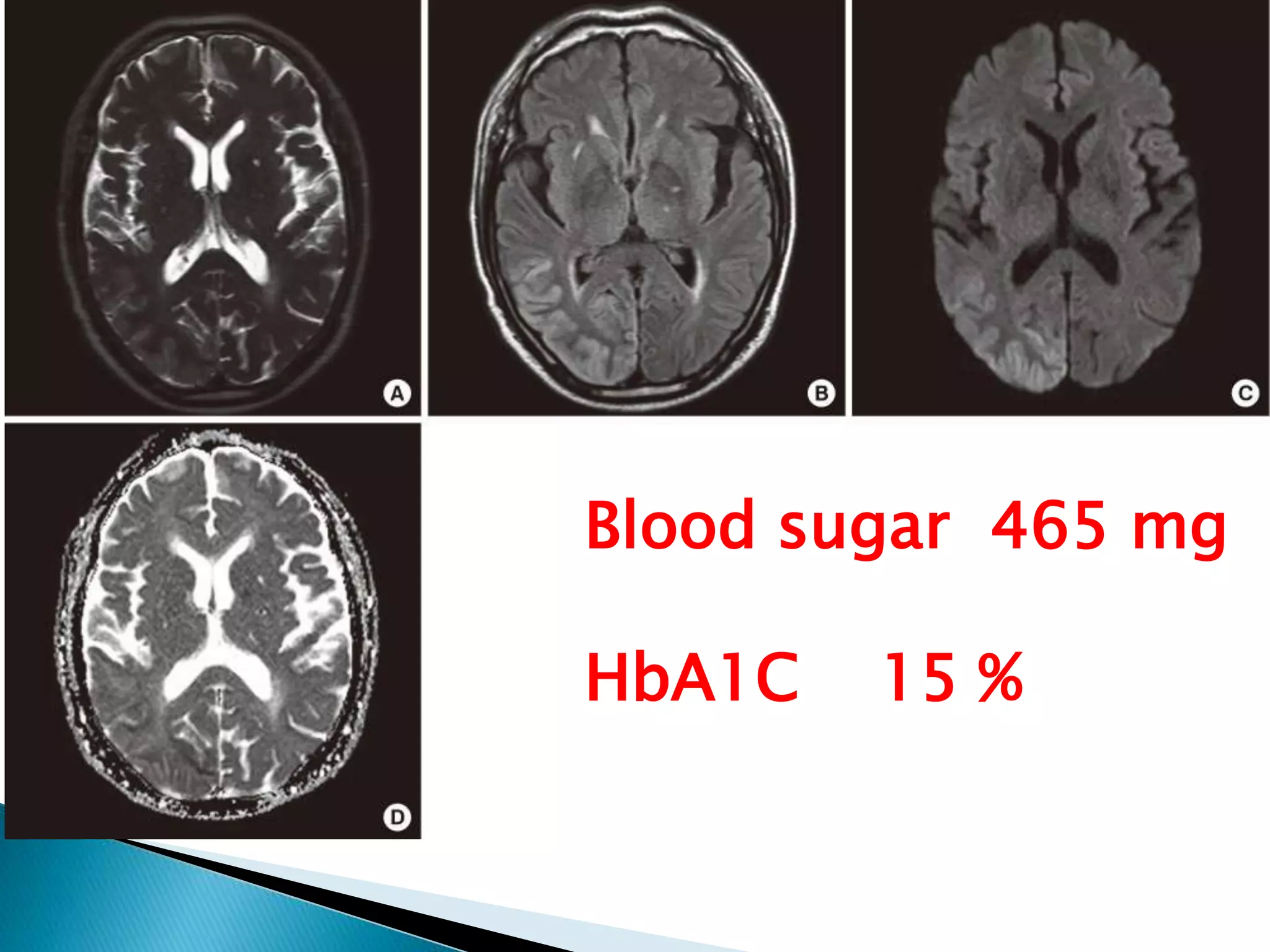
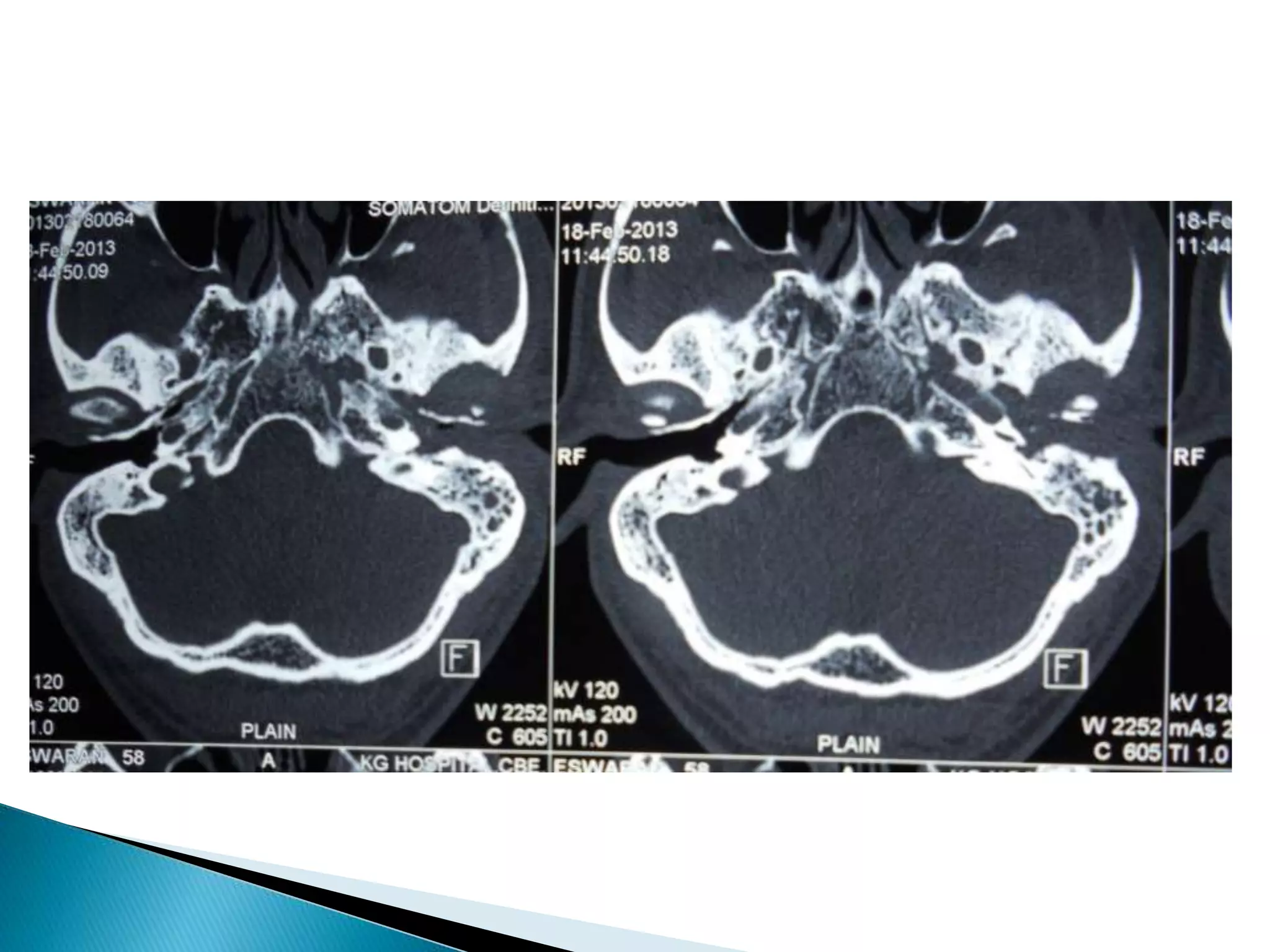
This document discusses various case presentations of diabetic patients. It begins with a case of hypoglycemia presenting with weakness and discusses appropriate treatment. It then covers various neurological manifestations of diabetes that can present including cranial neuropathies, peripheral neuropathies, and focal deficits related to hyperglycemia. Throughout various case examples are provided and key points are discussed such as appropriate workup, differential diagnoses to consider, and management strategies.












































![[2015] hepatic encephalopathy](https://cdn.slidesharecdn.com/ss_thumbnails/2015hepaticencephalopathy-151117004212-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)




















































































