Downloaded 45 times











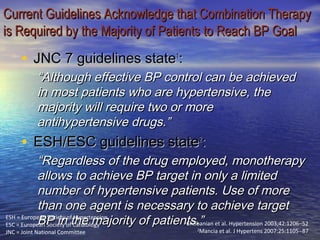

































































Hypertension is often difficult to treat effectively despite available drugs. Combination drug therapy is usually needed to control blood pressure, as monotherapy is only effective in 40-60% of patients. Using two drugs with different mechanisms of action can more effectively lower blood pressure than monotherapy alone. Common effective combinations include a diuretic paired with a renin-angiotensin system inhibitor, calcium channel blocker, or beta blocker. This helps control blood pressure through multiple pathways and limits side effects.























































