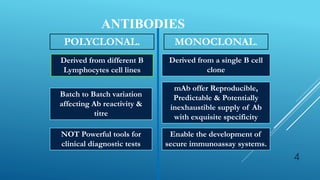
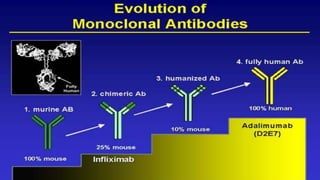
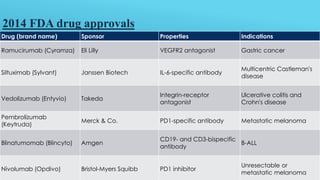
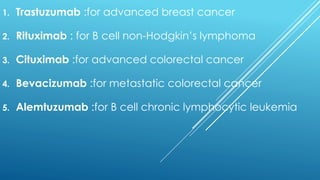
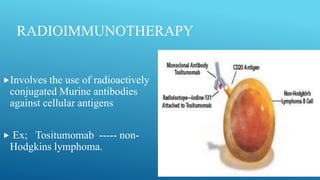
Monoclonal antibodies are derived from a single B cell clone and offer a reproducible and potentially inexhaustible supply of antibodies with exquisite specificity. They have enabled the development of more secure immunoassay systems and powerful clinical diagnostic tests. Monoclonal antibodies can be classified as naked antibodies or conjugated antibodies attached to drugs, toxins, or radioactive atoms to selectively target diseases. They have various mechanisms of action including blocking target antigens and inducing cytotoxicity, and are used to treat cancers, autoimmune disorders, and transplant rejection.








![Monoclonal antibodies [autosaved]](https://image.slidesharecdn.com/monoclonalantibodiesautosaved-150310003637-conversion-gate01/85/Monoclonal-antibodies-autosaved-41-320.jpg)