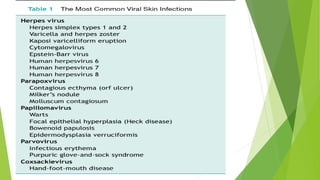
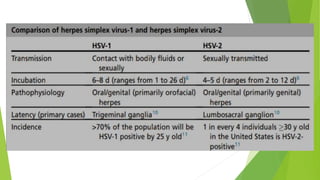
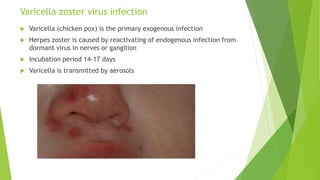
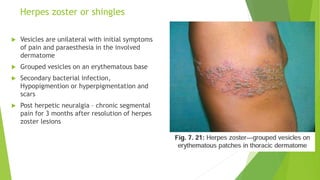
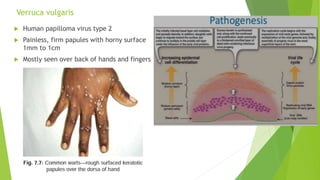
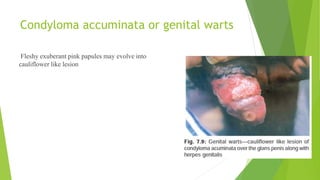
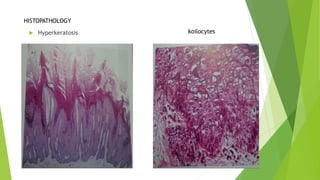
This document summarizes several common viral skin infections: herpes simplex virus causes cold sores and genital herpes; varicella zoster virus causes chickenpox and shingles; human papillomavirus causes warts and genital warts; molluscum contagiosum virus causes molluscum contagiosi; and enteroviruses can cause hand, foot, and mouth disease. It describes the causative viruses, symptoms, signs, treatments, and microscopic findings of these infections. Measles is also mentioned as a viral exanthem causing a maculopapular rash preceded by cough, runny nose, and conjunctivitis with Koplik's spots in the







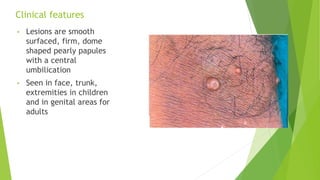
![Molluscum contagiosum
Pox virus [molluscum contagiosum
virus genotype 1(most
common),2(common in hiv patients),3
and 4]
Affects children, adults with sexually
transmitted disease and
immunocompromised patients
Skin to skin transmission, contact with
fomites, sexual transmission or auto
inoculation
Incubation period – 14 to 50 days](https://image.slidesharecdn.com/viralinfectionsderm-230912170739-7653a30a/85/viralinfectionsderm-pptx-22-320.jpg)



















![1.1.2. viral infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-2-viralinfectionsofskincompatibilitymode-120714004456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































