Moisturizers An Essential Component in Eczema Management
•
1 like•913 views

Eczema, also known as atopic dermatitis, is a skin condition characterized by a defective skin barrier that causes dryness, cracks, and easy penetration of allergens. The stratum corneum lipid layer is defective, resulting in water loss from the skin and increased susceptibility to irritants. Topical corticosteroids are commonly used to treat flare ups, while emollients are the foundation for long term management by helping repair the skin barrier. Proper skin cleansing and moisturization are also important to prevent exacerbation of eczema symptoms.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Moisturizers An Essential Component in Eczema Management
Similar to Moisturizers An Essential Component in Eczema Management (20)
More from Moch Kurniawan
More from Moch Kurniawan (20)
Moisturizers An Essential Component in Eczema Management
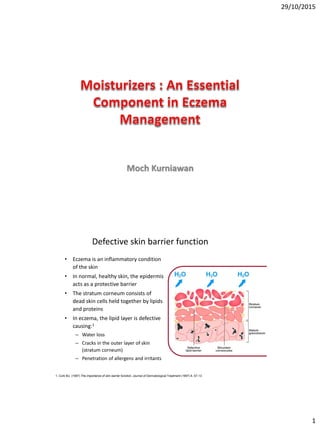
- 1. 29/10/2015 1 Moch Kurniawan Defective skin barrier function • Eczema is an inflammatory condition of the skin • In normal, healthy skin, the epidermis acts as a protective barrier • The stratum corneum consists of dead skin cells held together by lipids and proteins • In eczema, the lipid layer is defective causing:1 – Water loss – Cracks in the outer layer of skin (stratum corneum) – Penetration of allergens and irritants 1. Cork MJ. (1997) The importance of skin barrier function. Journal of Dermatological Treatment (1997) 8, S7-13
- 2. 29/10/2015 2 Allergy 2006: 61: 969–987
- 3. 29/10/2015 3 www.eczemahelp.ca *Robin Marks, Anne Plunkett, Kate Merlin, Nicole Jenner, Atlas of Common Skin Disease. Department of Dermatology, St Vincent’s Hospital, Melbourne, Australia, 1999. Prevalence of Atopic Dermatitis over all ages
- 4. 29/10/2015 4
- 5. 29/10/2015 5 Color Textbook of Pediatric Dermatology, 4th Edition. Infantile type Childhood type Adult type Face, scalp, trunk, extensor surfaces of extremities Flexural folds of ext (antecubital, popliteal fossa) neck, ankles Upper arms, back, wrists, hands, fingers, feet, toes
- 6. 29/10/2015 6 Atopic eczema affects quality of life Adapted from Jenner N et al. AustralasJ Dermatol 2004; 45(1): 16–22. 36 28 15 21 40 45 0 5 10 15 20 25 30 35 40 45 50 Spent >10 min/day applying treatments Influenced the clothes they wore Problems with treatment Felt embarassed by their skin Using 4 or more products Itchy, sore, painful or stinging Percentage of Patients (n = 85) Therapeutic objectives for atopic dermatitis Reduce signs and symptoms; Prevent or reduce recurrences Provide long-term management by preventing exacerbation; Modify the course of the disease Dr C. Ellis et al British Journal of Dermatology 2003; 148 (Suppl. 63): 3–10
- 7. 29/10/2015 7 The Consensus Conference on Pediatric Atopic Dermatitis Role of Emollients • Useful as first-line agents • Ointment preferred over creams • Frequent application recommended because of their short duration of action (6 hours) General Measures • Avoidance of irritating fabrics such as wool or synthetic in favor of cotton clothing Topical Steroids • Once or twice daily use of low- to medium-potency topical steroids as first-line therapy for disease exacerbations • Once controlled, topical steroids should be withdrawn or tapered to less potent or less frequent (twice weekly) application • Steroids can be used safely if monitored appropriately Oral Steroids • Avoid use of systemic steroids because of their side effects Topical non-steroidal immunosuppressive therapies (eg, tacrolimus and pimecrolimus) • Useful as intermittent, second-line therapy for moderate to severe AD (tacrolimus) or mild to moderate AD (pimecrolimus) • Not approved for children less than 2 years of age • Coordinated with sun protection because of concerns Source: Eichenfield LF, HanifinJM, Luger TA, et al. Consensus Conferenceon PediatricAtopic Dermatitis. J Am Acad Dermatol. 2003;49:1088-1095.
- 9. 29/10/2015 9
- 10. 29/10/2015 10 Emollients The most fundamental step in fighting atopic eczema is re-hydration The principle mode of action of emollients is improving the depleted lipid barrier of the skin thus reducing skin water loss Reduce eczema flare ups and the need of topical steroids PrimaryCare DermatologySociety & British Association of Dermatologists. Guidelinesfor the management of atopic eczema. October 2009. Cork MJ. (1997) The importance of skin barrier function. Journal of DermatologicalTreatment (1997) 8, S7-13 Prodigy – Quick Reference Guide. Emollients. [Online]. (URL www.prodigy.nhs.uk/Eczema-atopic). (Accessed 11 December 2006). 3 Stages of Emollient use in skin repair
- 11. 29/10/2015 11 Emollients must be applied regularly and frequently… • Every day, even when the skin looks clear • In conjunction with other treatments during flare-ups • Every 3-4 hours • Helping patients to build emollient application into their daily routine can make it easier for them to adhere to …and in the right quantities • To get the most out of emollients, patients need to know how much they should use • Illustrating how much emollient your patients should apply can be helpful • Most pumps dispense approximately 4g Adapted from Dunning G. Nursing Times 2005; 101 (4): 55-56
- 12. 29/10/2015 12 Complete emollient therapy • Giving patients a combination of different formulations and sizes can encourage them to use them regularly, frequently and in sufficient volume, for example: – An ointment tub for use on severe areas or at night – A large cream pump dispenser for daily moisturising and washing – A smaller tube of cream or ointment for use when out and about – A bath substitute as an alternative to cosmetic wash products Prescribing emollients in sufficient volume • 250-500g per week for children3 – Between 2-4 500g pump dispensers per month • 600g per week for adults1 – 4 x 500g pump dispensers per month • Pump dispensers are a good way to help patients: – Use the correct volumes – Reduce cross contamination 1. Primary Care Dermatology Society & British Association of Dermatologists. Guidelines for the management of atopic eczema. October 2009. 3. NICE (2007) Clinical Guideline 57, London, December 2007
- 13. 29/10/2015 13 Cleansing Skin cleansing • Ordinary soap can dry the skin and worsen itching. • Ordinary soap contains sodium lauryl sulphate (SLS) which further aggravate and irritate skin. • Ordinary soap can cause flare up and block the effects of the treatment. • The key to cleansing in children with atopic dermatitis is to be gentle due to the damaged, fragile stratum corneum.
- 14. 29/10/2015 14 Skin cleansing • Cleansing, with water, soap or a liquid cleanser, will affect the moisture skin barrier • Soap will bring about the greatest changes to the barrier and increase skin pH • Liquid facial cleansers are gentler, effecting less disruption of the barrier, with minimal change to skin pH, and can provide people with a cleanser that is a combination of surfactant classes, moisturizers and acidic pH in order to minimize disruption to the skin barrier Skin Therapy Letter • Editor: Dr. Stuart Maddin • Vol. 8 No. 3 • March 2003 Skin cleansing • The dry skin of eczema is not caused by a lack of oil in the skin, but because the skin barrier is damaged, so that the skin cannot retain water. • This is why a skin regimen focused on bathing and moisturizing is your first defence against eczema flare-ups www.eczemahelp.ca
- 15. 29/10/2015 15 Skin cleansing • Moisturising, mild pH-neutral or acidic cleansers should be used • The use of bath oils free of fragrances and emulsifying agents is also recommended. • Soaps and bubble baths should be avoided. • Bathing time should not exceed 15 to 20 minutes • Immediately after showering or bathing, a moisturiser should be applied. http://skincare.dermis.net/content/e04erkrankt/e617/e620/index_eng.html IRRITANTS Sodium Lauryl Sulfate (SLS) & Sodium Laureth Sulfate (SLES)
- 16. 29/10/2015 16 The skin's natural moisturizing factors are amino acids The skin's natural moisturizing factors are amino acids
- 17. 29/10/2015 17 Very mild and hypoallergenic. Weakly acidic, similar to the pH level of the skin, leaving the skin without a taut feeling. Mild and gentle to the hair without leaving it dry and coarse. Amisoft is less irritant than SLS / SLES 0 1 2 3 0 1 2 3 4 5 Days Reading Sodium Lauryl Sulfate Amisoft Water A five day human patch test N=72 (age : 19-72, 30 men & 42 women) Score Symptoms 0 No reaction 0.5 Slight erythema 1.0 Clear erythema & hardening 2.0 Erythema & vesiculation or dryness AJINOMOTO Co., Inc. AminoScience Lab. 2003.09.16.
- 18. 29/10/2015 18 Prevention •help soften the skin and lock in moisture •should be applied after bathing and frequently throughout the day Apply emollients and moisturizers •If the results of the patch testing indicate an allergy, the patient should avoid all items that contain the allergen (substance causing the allergy) Avoid allergens •The dermatologist will talk about options for avoiding the substance(s) that is irritating the skin. Avoid irritants •If the patient wears gloves at work, it is important to realize that substances on the hands can get inside the gloves and irritate the skin, especially when more than one substance gets inside the gloves Change work habits Effective formulations for all types of skin
- 19. 29/10/2015 19 www.eczemahelp.ca The role of topical steroids • Topical steroids are widely used to relieve acute symptoms and clear flare-ups • They come as creams and ointments, and in a range of strengths – So that patients can be given one that is ideal for the severity and location of their eczema • Topical steroids should be applied to inflamed areas only and used twice a day at most • They should be used sparingly and only for as long as is necessary to clear up the flare – Fingertip units can be a useful way for patients to measure doses
- 20. 29/10/2015 20 Prescribing topical steroids • Topical steroids are usually prescribed using a step-wise approach:3 – Starting with the correct potency based on the severity of eczema – Stepping down as the severity decreases – Or stepping up as required • The face and neck should normally only be treated with mild steroids – adverse effects are more likely in areas where the skin is thinner 3. NICE (2007) Clinical Guideline 57, London, December 2007 Akdis et al. J ALLERGY CLIN IMMUNOL JULY 2006
- 22. 29/10/2015 22