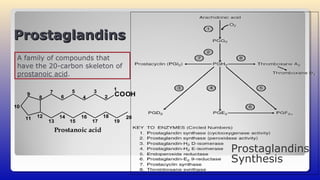

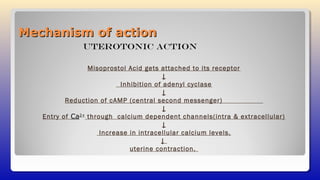

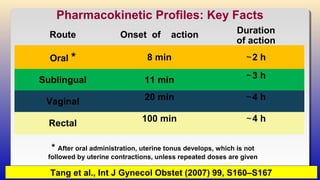
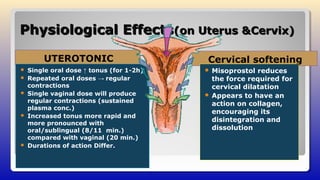
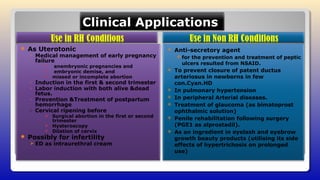








Misoprostol is a prostaglandin E1 analogue discovered in 1973, primarily used in obstetrics for uterine contractions, cervical softening, and abortion. It has shown effectiveness in preventing postpartum hemorrhage and facilitating labor induction, while its pharmacokinetics reveal variability in absorption and metabolic pathways. Despite some side effects, misoprostol is recognized for its significant benefits in low-resource settings and its role in managing major causes of maternal mortality.



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
