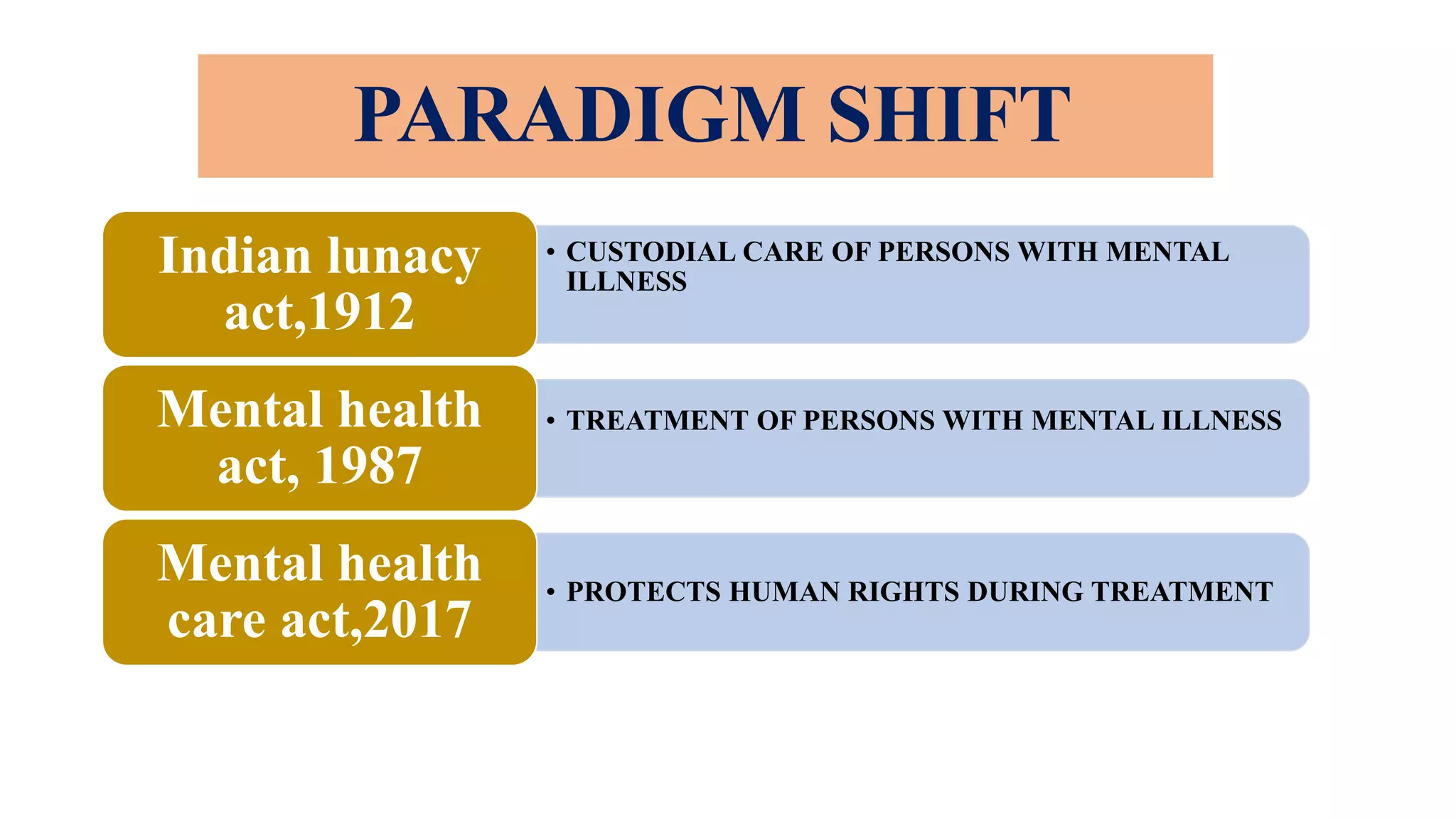
This document summarizes the history and key aspects of mental health care legislation in India. It discusses the Indian Lunacy Act of 1912, which was replaced by the Mental Health Act of 1987. However, both acts were criticized for their custodial and rights-violating nature. The Mental Health Care Act of 2017 was passed to address these issues and protect the human rights of those with mental illness based on recommendations from the Indian Psychiatric Society and India's ratification of the UN Convention on the Rights of Persons with Disabilities. The 2017 act includes provisions on advance directives, nominated representatives, rights of those with mental illness, registration of mental health establishments, and mental health review boards.


![And On the same day i.e. 29th May 2018 -3 important laws/rules were also
planned, drafted, and notified
1. Mental Health Care Rules 2018 [Rights of Person with Mental Illness under
section 121(1) and (3)]
2. Mental Health Care Rules 2018 for Central Mental Health Authority(CMHA) and
Mental Health Review Board (MHRB) under section 121 (1) and (3)
3. Mental Health Care Rules 2018 for State Mental Health Authority under section
121 (1) and (4)](https://image.slidesharecdn.com/mhca2017final-230806151502-a233ab8e/75/MHCA-2017-FINAL-pptx-10-2048.jpg)
![ON 16TH AUGUST 2019-
1. Guidance document for assessment of Mental Capacity under [MHCA,2017-
Section 81(1)]
2. List of essential drugs under mhca 2017- sec. 8(10)
18th DECEMBER. 2020-
1. Central Mental Health Regulation was also notified under MHCA 2017- Section
122](https://image.slidesharecdn.com/mhca2017final-230806151502-a233ab8e/75/MHCA-2017-FINAL-pptx-11-2048.jpg)