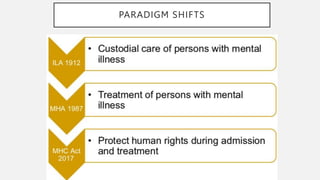
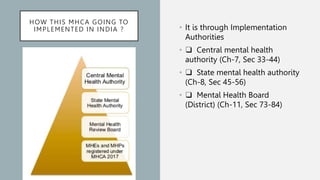
This document summarizes key aspects of the Mental Healthcare Act, 2017 in India. It outlines the objectives of providing and protecting mental healthcare rights. It describes the implementation authorities at the central, state, and district levels. Key shifts include a focus on care over custody, and protecting human rights. Obligations of mental health establishments include registering with authorities, ensuring minimum standards, and adhering to patient rights. Admission and discharge procedures are detailed to respect patient capacity and autonomy.







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

